


The prevalence of obesity and overweight in Northeastern Iran
- Dezful University of Medical Sciences, Dezful, Iran
- Refractive Errors Research Center, School of Paramedical Sciences, Mashhad University of Medical Sciences, Mashhad, Iran
- Noor Research Center for Ophthalmic Epidemiology, Noor Eye Hospital, Tehran, Iran
- Department of Optometry, School of Paramedical Sciences, Mashhad University of Medical Sciences, Mashhad, Iran
- Department of Medical Surgical Nursing, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Abstract
Objective: The aim of this study was to assess obesity and overweight by WHO criteria in Mashhad, Iran.
Method: This cross-sectional study was performed on 4453 people from Mashhad in 2009. Comprehensive data of age, height, weight, education, and marriage was collected. Overweight and obesity were calculated according to the body mass index (BMI).
Results: A total of 1828 participants entered study, of whom 70.4% were women. The mean age of the population was 39.8±13.5 years. The prevalence of overweight and obesity was 36.5% (95% CI 34.3-38.6) and 16.9% (95% CI 15.1-18.8), respectively. The prevalence of overweight was 39.0% in men and 35.4% in women which increased significantly by age (P<0.001 & OR=1.055). The prevalence of obesity in men and women was 12.3% and 18.9% respectively which showed women had a significantly higher risk (P<0.001). The risk of overweight and obesity was higher in married but lower in educated people.
Conclusion: This study showed a rapid increase in obesity and overweight, especially in women, in Mashhad population as a sample of the Iranian society. Attention to preventive and education plans should be the priority of health policies.
Background
The increasing trend of non-communicable diseases is one of the greatest public health challenges, especially in developed countries 1. Obesity is one of the most important risk factors of cardiovascular diseases, diabetes, and cancer, and is the 5cause of mortality and morbidity worldwide 2. According to the WHO reports, more than 1.5 billion people aged 20 years and older are obese in the world 3. More than 65% of the world population lives in countries where most people die of obesity and overweight. Moreover, 44% of the burden of diabetes and 23% of the burden of cardiac ischemic diseases in attributed to obesity 4. Many studies underline the importance of obesity every year 567 . Based on the latest reports of the WHO, the BMI has had an increasing trend since 1980; for this reason, its estimate for the coming years is concerning 8. According to the WHO reports, the highest prevalence of obesity is observed in American and European countries followed by the countries located in the eastern Mediterranean region and the lowest prevalence is seen in South African countries 9. Iran is one of the densely populated countries in the Eastern Mediterranean region. In a report on the trend of obesity and overweight, Esteghamati reported an increasing trend between 1999 and 2007 10. According to the findings of this study, obesity can be the cause of a high percentage of non-communicable diseases in Iran in recent years 10. This study suggested that periodic studies in Iran could provide health managers with information on the epidemic of obesity in different parts of the country; in addition, information on the status of obesity in Iran can help to have an estimate on the incidence of cardiovascular diseases and even cancers that result from obesity 10. Furthermore, considering the variety in the ethnicity, socioeconomic status, educational level, and even the occupational status of the Iranian population, different studies are required to determine the status of obesity in different groups 111213. Due to the importance of obesity and since it is a major public health concern worldwide, we decided to evaluate the prevalence of obesity and overweight in a population based study according to the WHO criteria.
Methods
This cross sectional population based study was conducted in Mashhad, northeast of Iran. The target population of this study was the over-1-year population of Mashhad. The population of Mashhad is 2,451,712 according to the 2005 census. The city of Mashhad has 11 municipality districts, which were considered as strata. The random stratified cluster sampling method was used to select the select the participants. The number of people in each strata was considered proportion of that strata to whole population in sampling.
A total of 120 clusters of the blocks determined by the Statistics Center of Khorasan Razavi Province were randomly selected. The first house number of each cluster was considered the head cluster. In each cluster, sampling continued systematically for up to 10 households. After introducing themselves and explaining the importance of the project to the households and completing a demographic questionnaire, the interviewers invited the households to the Optometry Clinic of Mashhad University of Medical Sciences for a complete examination. If a household declined the invitation, the next household according to the house number was invited. Accordingly, 10 households were invited to the study systematically in a clock-wise fashion. The travel costs of the households were covered by the research team.
After selecting the households and their visit to the Optometry Clinic, their demographic characteristics and history of ophthalmic examination were evaluated through an interview. The height and weight of the participants were measured after the interview.
In this study, the height of the participants was measured with a plastic tape measure attached to the wall. The height was measured in the standing position with shoes removed and 5 body points making contact with the wall. A SECA digital scale was used to weight measurement.
Definitions
The BMI was used to calculate obesity and overweight. The BMI was calculated as the body mass (kg) divided by the square of the body height (m). A BMI of 25-29.9 was considered overweight and a BMI ≥30 was considered obese. To calculate the level of obesity, a BMI of 30-34.9, 35-39.9, and ≥40 was considered obesity grade 1, obesity grade 2, and obesity grade 3, respectively.
Ethical Considerations
After the households visited the clinic willingly, the protocol of the study was again explained to the head of the household explicitly. Then, if the household was willing to participate in the study, informed consent was obtained from the head of the household. The consent form included the commitments of the research team to confidentiality and anonymity of the data. The protocol of the study was approved by the Ethics Committee of Mashhad University of Medical Sciences.
Statistical Analysis
The prevalence of overweight and obesity is reported as percentage with 95% CI. The method of cluster sampling was considered when calculating 95% CI. Simple and multiple logistic regression models were used to investigate the relationships. Overweight and obese individuals were compared with those whose BMI was below 25 to evaluate the correlations. When there was not a linear relationship, continues variableswere dummy and a group was considered as a reference for comparison with other groups.
Results
Of 4453 participants who were invited, 70.4% participated in the study. Of them, 1828 were 20 years and older whose data was analyzed in this study. Female participants comprised 70.4% of the study population. The mean age of the participants was 39.8±13.5 years (range: 20-90 years). The mean BMI standardized according to age and gender was 25.7 (95% CI 25.4-25.9). Figure 1shows the distribution of BMI in the study population. The BMI was 25.6 in women and 25.4 in men, which had a significant difference (P<0.001). The relationship was also observed after adjusting for age. The BMI increased significantly until 60 years of age and then decreased; this trend was true in both sexes (Figure 2).
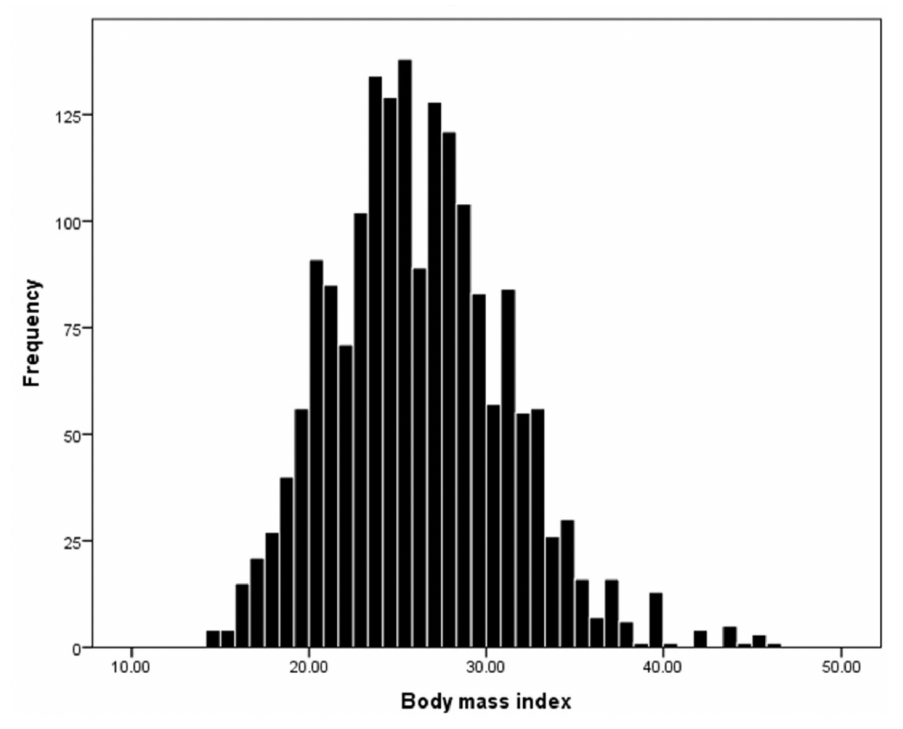
Distribution of BMI in the study population.
The prevalence of overweight and obesity in the study population according to the evaluated variables
| Overweight | Obese | |
| % (95%CI) | % (95%CI) | |
| Male | ||
| 20-29 | 35.1(26.1 - 44.20) | 7.2(2.3 - 12.1) |
| 30-39 | 43.9(34.4 - 53.30) | 11.4(5.5 - 17.3) |
| 40-49 | 35.2(27.4 - 43) | 17.9(11.7 - 24.1) |
| 50-59 | 39(29.2 - 48.90) | 10.5(4.7 - 16.2) |
| 60+ | 46(32.4 - 59.60) | 12.7(4.8 - 20.6) |
| Total | 39(34.6 - 43.50) | 12.3(9.5 - 15) |
| Female | ||
| 20-29 | 23.9(19.6 - 28.30) | 10(6.7 - 13.3) |
| 30-39 | 38.6(33.2 - 43.90) | 21.2(16.6 - 25.7) |
| 40-49 | 44.8(39.8 - 49.80) | 25.2(20.2 - 30.1) |
| 50-59 | 38.3(29.7 - 46.90) | 22.8(16 - 29.5) |
| 60+ | 34.1(24 - 44.30) | 19.5(10 - 29) |
| Total | 35.4(32.8 - 38) | 18.9(16.7 - 21.1) |
| Both gender | ||
| 20-29 | 26.5(22.5 -30.40) | 9.4(6.5 - 12.2) |
| 30-39 | 39.9(35.1 - 44.60) | 18.7(15.1 - 22.4) |
| 40-49 | 41.7(37.5 - 45.80) | 22.8(18.8 - 26.9) |
| 50-59 | 38.6(32.4 - 44.90) | 18(12.9 - 23.1) |
| 60+ | 39.3(31.5 - 47.10) | 16.6(10.6 -22.5) |
| Total | 36.5(34.3 - 38.60) | 16.9(15.1 - 18.8) |
| Mariage status | ||
| Single | 17.9(12.4 - 23.40) | 5.3(2.1 - 8.6) |
| Married | 38.9(36.5 - 41.20) | 18.4(16.4 - 20.5) |
| Educational level | ||
| Illiterate | 37.3(30.2 - 44.30) | 17.7(12.5 - 22.9) |
| High school diploma or less | 37(34.4 - 39.60) | 18.1(15.8 - 20.4) |
| Associate degree | 33.7(29 - 38.40) | 13.9(10.3 - 17.4) |
| Masters degree or more | 43.8(25.4 - 62.10) | 3.1(-3.00 - 9.3) |
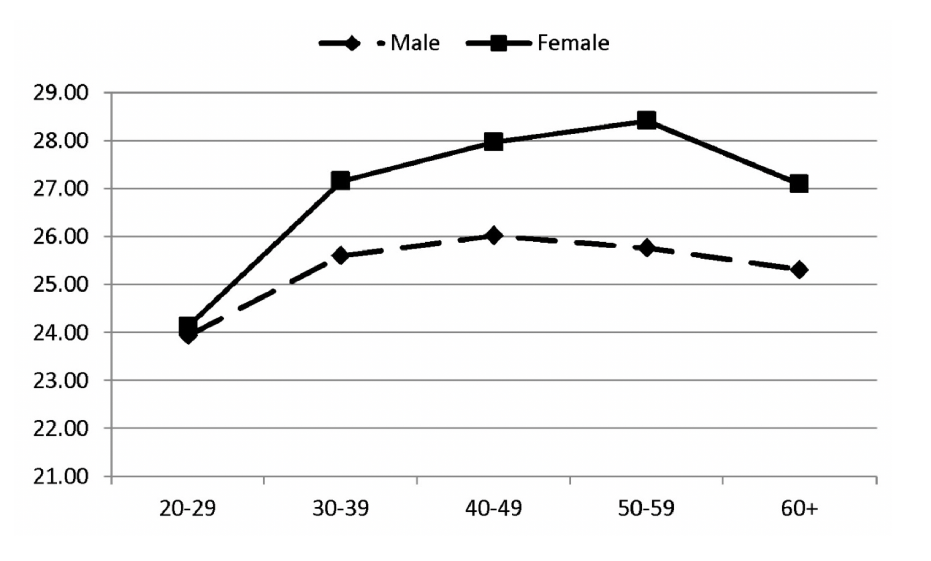
BMI in different age groups of men and women.
The relationship of obesity and overweight with study variables in a multiple model
| Overweight | Obese | ||||
| Or (95%ci) | P-value | Or (95%ci) | <0.001 | ||
| Gender | Male/Female | 1.04 (0.80 - 1.35) | 0.795 | 1.98 (1.44 - 2.72) | |
| Age | 20-29 | 1 | 1 | <0.001 | |
| 30-39 | 1.75 (1.25 - 2.45) | <0.001 | 2.36 (1.50 - 3.72) | <0.001 | |
| 40-49 | 2.14 (1.55 - 2.96) | <0.001 | 3.59 (2.24 - 5.77) | 0.002 | |
| 50-59 | 1.60 (1.10 - 2.31) | 0.013 | 2.40 (1.37 - 4.20) | 0.017 | |
| 60+ | 1.70 (1.07 - 2.69) | 0.023 | 2.41 (1.17 - 4.96) | ||
| Educational level | Illiterate | 1 | 1 | 0.278 | |
| High school diploma or less | 1.20 (0.80 - 1.81) | 0.385 | 1.35 (0.78 - 2.32) | 0.337 | |
| Associate degree | 1.20 (0.76 - 1.91) | 0.436 | 1.36 (0.72 - 2.57) | 0.438 | |
| Masters degree or more | 1.58 (0.75 - 3.31) | 0.228 | 0.41 (0.04 - 3.85) | ||
| Marital status | Single | 1 | 1 | 0.002 | |
| Maried | 2.69 (1.73 - 4.20) | <0.001 | 3.24 (1.56 - 6.75) |
Overweight
The prevalence of overweight was 36.5% (95% CI 34.3-38.6) in our study. The prevalence of overweight was 39.0% (95% CI 34.6-43.5) in men and 35.4% (95% CI 32.4-38.0) in women. Logistic regression showed no correlation between sex and overweight (P=0.782). This relationship was observed after adjusting for age (P=0.658). The prevalence of overweight did not have a linear relationship with age. According to Table 1, the prevalence ofoverweight increased from 20 to 49 years of age and then decreased thereafter. Logistic regression showed that the prevalence of overweight increased from 20 to 49 years of age (OR=1.055, P<0.001). The changes of overweight did not have a significant relationship with age after 49 years of age (P=0.779). The prevalence of overweight did not have a significant correlation with the level of education. Chi-2 showed no significant difference between the educational level and overweight (P=0.367). The prevalence of overweight was significantly higher in married participants; the prevalence of overweight was 17.9% in single and 38.9% in married participants. Simple logistic regression showed that the odds of overweight was 3.3 times greater in married versus single participants (P<0.001). The results of the multiple regression model are presented in Table 2. Accordingly, age and marital status had a significant relationship with overweight.
Obesity
The prevalence of obesity was 16.9% (95% CI 15.1-18.8). The prevalence of obesity was 12.3% (95% CI 9.5-15.0) in women and 18.9% (95% CI 16.7-21.1) in men. According to the simple logistic regression model, the odds of obesity were significantly higher in women (OR=1.6, 95% CI 1.2-2.2 P<0.001). The prevalence of obesity increased significantly from 9.5% in participants aged 20-29 years to 22.8% in the age group 40-49 years (P<0.001); however, the changes of obesity were not significantly correlated with age after 50 years of age (P=0.904). This relationship was true in both sexes. According to Table 1, the lowest prevalence of obesity was observed in individuals with a master’s degree or higher. Logistic regression showed that the odds of obesity were higher in individuals with a master’s degree or higher versus illiterate participants (OR=1.6, 95% CI 0.11-0.96 P=0.046). The prevalence of obesity was significantly higher in married people (P<0.001). Table 2 shows the results of the multiple logistic regression model. According to Table 2, female sex, age, and marital status had a significant correlation with obesity.
Discussion
In this study, we reported the prevalence of obesity and overweight by sex, marital status, and educational level in a population of Mashhad, as a representative of the Iranian population, according to the WHO criteria.
According to our results, 36.5% of the participants were overweight and 16.9% were obese. A review of the previous studies shows a lower prevalence of overweight and obesity in Mashhad when compared with Gorgan, Tehran, and Shiraz in both sexes while its prevalence was higher in Isfahan 1415161718. However, the prevalence of overweight and obesity in Mashhad is lower than the whole country; a national study that evaluated the BMI of Iranian men and women (BMI≤25) reported that the prevalence of overweight and obesity was 42.8% and 57% 19. In 2008, the WHO reported a prevalence of 48.0% for overweight and 7.18% for obesity in the Middle East. A number of studies have reported a high prevalence of obesity and overweight in neighboring countries of Iran like the KSA, Turkey, and Oman but the prevalence is lower than countries like Italy, China, and Portugal 20212223242526 . These studies indicate that Iran, like its neighbors and as a developing country, is undertaking a socioeconomic transition; access to food and high calorie diets has increased in the past 10 years and physical activity has decreased due to the use of public and personal vehicles 27. These changes, along with the prevalence of obesity, result in energy imbalance and increased burden of different diseases resulting from obesity; cardiovascular diseases are now the first cause of mortality and morbidity due to non-traumatic events in Iran 28. However, the difference in the prevalence of obesity also depends on factors such as diet, access to food products, education level, and GDP. The prevalence of obesity and overweight is on the rise in Europe and America; According to a WHO report, the highest and lowest prevalence of obesity is observed in North America and Southeast Asia, respectively. In another study, Flegal et al. reported a prevalence of 68.8% for overweight and 35.7% for obesity in Americal population aged 20 years and over 29. Concerns about the epidemic of obesity among the young generation are a major public health challenge because it increased the burden of the diseases incurs heavy costs on the society and increases the risk of atherosclerotic diseases and diabetes in the future. Therefore, preventive measures, increasing public awareness and knowledge, and physical activity are recommended to lower the prevalence of obesity. According to a study performed in a Japanese young population between 2003 and 2009, lifestyle modification decreased the prevalence of overweight and obesity 30
Our results showed that the prevalence of obesity and overweight was higher in women and men, respectively. These prevalence rates were higher than the finding of a national study that reported a prevalence of 11.1% for obesity in Iranian men 19. Farhadian et al. also reported that the prevalence of obesity in men residing in Khorasan razavi Province was higher than other provinces The results of the studies performed in Tehran, Golestan, Mazandaran, and Shiraz indicate the higher prevalence of obesity and overweight in women across the country 111617183132.eports of the rather high prevalence of overweight and obesity in women living in neighboring countries of Iran like Oman, Kuwait, and Turkey; for example, 62.65% of the women in Saudi Arabia suffer from overweight 20212223. The reason could be that their lifestyle is similar to the lifestyle of Iranian women; most women in the Middle East are housewives and have little physical activity which is a major risk factor of obesity. In this regard, the prevalence of overweight and obesity is 4% and 10% lower respectively in Iranian female clerks that have more physical activity than their housewife counterparts 33. There is anotr reason to doubt the results of the above-mentioned studies. Most of these study collected information through census and door-to-door interview and as mentioned earlier, women spend most of their time at home in these countries and as a result, the information of the height and weight of other members of the household may not have been collected accurately. As mentioned in Results, the prevalence of obesity and overweight was higher in married versus single participants. A number of studies performed in Iran and other countries have confirmed the higher prevalence of Overweight in married people in both sexes 1134353637. The reason is not yet clear but cultural reasons like persuading the spouse to dine together or more attention to meals could be involved 16.
It was mentioned earlier that the prevalence of overweight and obesity was lower in people with higher education (master’s degree and higher) versus people with lower education. Previous studies 2631383940 ht people with higher education, in addition to having a correct insight and attitude toward the complications of obesity and observing an appropriate diet, have a higher income and spend money on appropriate foods more easily. The results of a cohort study on healthy women with normal BMI in England showed that they spent about 1000£ on buying high fiber, protein, and vitamin foods while the opposite was observed in people with a low income that spent most of their money on unhealthy fast foods containing high amounts of fat and carbohydrates, resulting in an increased risk of obesity 2631383940. However, anothported that people witan academic education are more prone to obesity because they mostly have office jobs and a sedentary lifestyle as compared to illiterate or low educated people who are mostly labors requiring a lot of energy.
Conclusions
According to the results of our study, the rising trend of the prevalence of overweight and obesity is concerning in the urban population of Mashhad. Due to the association of overweight and obesity with cardiovascular diseases and diabetes, it seems that more attention should be paid to obesity and overweight in Mashhad, which can be regarded as a necessity and a health system priority in Mashhad. For this reason, preventive measures like enhancing the socioeconomic status of the target population, increasing their awareness, and providing them with education on nutrition should be considered as the main objectives of health managers in this regard.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License (CC-BY 4.0) which permits any use, distribution, and reproduction in any medium, provided the originalauthor(s) and the source are credited.
Ethics approval and consent to participate
Not to be applied.
Competing interests
The authors declare that they have no competing interests.
Funding
Not to be applied.