Open Access
Open Access Abstract
Objective: The aim of this study was to assess obesity and overweight by WHO criteria in Mashhad, Iran.
Method: This cross-sectional study was performed on 4453 people from Mashhad in 2009. Comprehensive data of age, height, weight, education, and marriage was collected. Overweight and obesity were calculated according to the body mass index (BMI).
Results: A total of 1828 participants entered study, of whom 70.4% were women. The mean age of the population was 39.8±13.5 years. The prevalence of overweight and obesity was 36.5% (95% CI 34.3-38.6) and 16.9% (95% CI 15.1-18.8), respectively. The prevalence of overweight was 39.0% in men and 35.4% in women which increased significantly by age (P<0.001 & OR=1.055). The prevalence of obesity in men and women was 12.3% and 18.9% respectively which showed women had a significantly higher risk (P<0.001). The risk of overweight and obesity was higher in married but lower in educated people.
Conclusion: This study showed a rapid increase in obesity and overweight, especially in women, in Mashhad population as a sample of the Iranian society. Attention to preventive and education plans should be the priority of health policies.
Background
The increasing trend of non-communicable diseases is one of the greatest public health challenges, especially in developed countries 1 . Obesity is one of the most important risk factors of cardiovascular diseases, diabetes, and cancer, and is the 5 th cause of mortality and morbidity worldwide 2 . According to the WHO reports, more than 1.5 billion people aged 20 years and older are obese in the world 3 . More than 65% of the world population lives in countries where most people die of obesity and overweight. Moreover, 44% of the burden of diabetes and 23% of the burden of cardiac ischemic diseases in attributed to obesity 4 . Many studies underline the importance of obesity every year 5 6 7 . Based on the latest reports of the WHO, the BMI has had an increasing trend since 1980; for this reason, its estimate for the coming years is concerning 8 . According to the WHO reports, the highest prevalence of obesity is observed in American and European countries followed by the countries located in the eastern Mediterranean region and the lowest prevalence is seen in South African countries 9 . Iran is one of the densely populated countries in the Eastern Mediterranean region. In a report on the trend of obesity and overweight, Esteghamati reported an increasing trend between 1999 and 2007 10 . According to the findings of this study, obesity can be the cause of a high percentage of non-communicable diseases in Iran in recent years 10 . This study suggested that periodic studies in Iran could provide health managers with information on the epidemic of obesity in different parts of the country; in addition, information on the status of obesity in Iran can help to have an estimate on the incidence of cardiovascular diseases and even cancers that result from obesity 10 . Furthermore, considering the variety in the ethnicity, socioeconomic status, educational level, and even the occupational status of the Iranian population, different studies are required to determine the status of obesity in different groups 11 12 13 . Due to the importance of obesity and since it is a major public health concern worldwide, we decided to evaluate the prevalence of obesity and overweight in a population based study according to the WHO criteria.
Methods
This cross sectional population based study was conducted in Mashhad, northeast of Iran. The target population of this study was the over-1-year population of Mashhad. The population of Mashhad is 2,451,712 according to the 2005 census. The city of Mashhad has 11 municipality districts, which were considered as strata. The random stratified cluster sampling method was used to select the select the participants. The number of people in each strata was considered proportion of that strata to whole population in sampling.
A total of 120 clusters of the blocks determined by the Statistics Center of Khorasan Razavi Province were randomly selected. The first house number of each cluster was considered the head cluster. In each cluster, sampling continued systematically for up to 10 households. After introducing themselves and explaining the importance of the project to the households and completing a demographic questionnaire, the interviewers invited the households to the Optometry Clinic of Mashhad University of Medical Sciences for a complete examination. If a household declined the invitation, the next household according to the house number was invited. Accordingly, 10 households were invited to the study systematically in a clock-wise fashion. The travel costs of the households were covered by the research team.
After selecting the households and their visit to the Optometry Clinic, their demographic characteristics and history of ophthalmic examination were evaluated through an interview. The height and weight of the participants were measured after the interview.
In this study, the height of the participants was measured with a plastic tape measure attached to the wall. The height was measured in the standing position with shoes removed and 5 body points making contact with the wall. A SECA digital scale was used to weight measurement.
Results
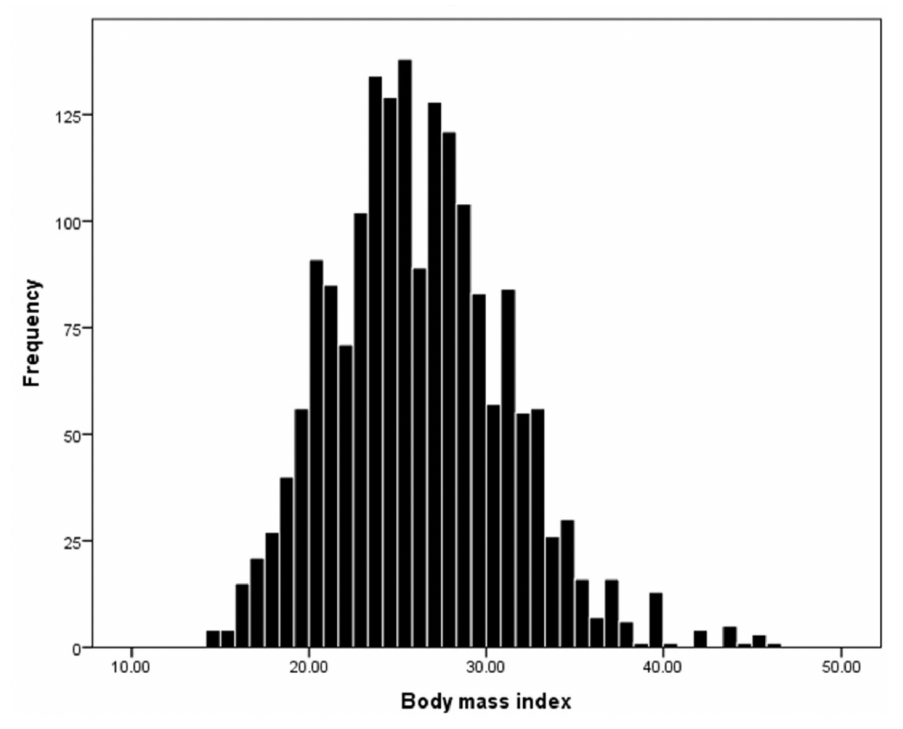
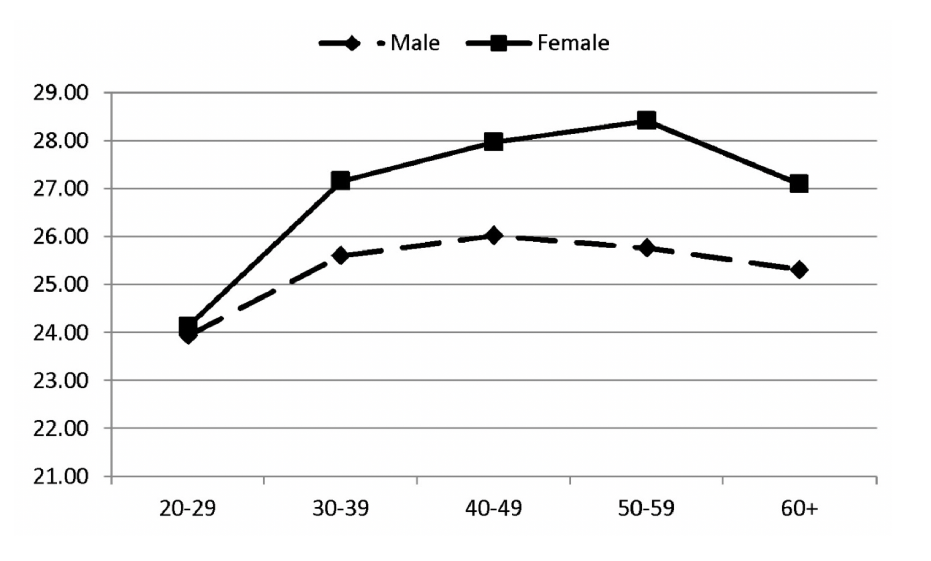
Of 4453 participants who were invited, 70.4% participated in the study. Of them, 1828 were 20 years and older whose data was analyzed in this study. Female participants comprised 70.4% of the study population. The mean age of the participants was 39.8±13.5 years (range: 20-90 years). The mean BMI standardized according to age and gender was 25.7 (95% CI 25.4-25.9). Figure 1 shows the distribution of BMI in the study population. The BMI was 25.6 in women and 25.4 in men, which had a significant difference (P<0.001). The relationship was also observed after adjusting for age. The BMI increased significantly until 60 years of age and then decreased; this trend was true in both sexes ( Figure 2 ) .
| Overweigh t | Obese | |
| % (95%CI) | % (95%CI) | |
| Male | ||
| 20-29 | 35.1(26.1 - 44.20) | 7.2(2.3 - 12.1) |
| 30-39 | 43.9(34.4 - 53.30) | 11.4(5.5 - 17.3) |
| 40-49 | 35.2(27.4 - 43) | 17.9(11.7 - 24.1) |
| 50-59 | 39(29.2 - 48.90) | 10.5(4.7 - 16.2) |
| 60+ | 46(32.4 - 59.60) | 12.7(4.8 - 20.6) |
| Total | 39(34.6 - 43.50) | 12.3(9.5 - 15) |
| Female | ||
| 20-29 | 23.9(19.6 - 28.30) | 10(6.7 - 13.3) |
| 30-39 | 38.6(33.2 - 43.90) | 21.2(16.6 - 25.7) |
| 40-49 | 44.8(39.8 - 49.80) | 25.2(20.2 - 30.1) |
| 50-59 | 38.3(29.7 - 46.90) | 22.8(16 - 29.5) |
| 60+ | 34.1(24 - 44.30) | 19.5(10 - 29) |
| Total | 35.4(32.8 - 38) | 18.9(16.7 - 21.1) |
| Both gender | ||
| 20-29 | 26.5(22.5 -30.40) | 9.4(6.5 - 12.2) |
| 30-39 | 39.9(35.1 - 44.60) | 18.7(15.1 - 22.4) |
| 40-49 | 41.7(37.5 - 45.80) | 22.8(18.8 - 26.9) |
| 50-59 | 38.6(32.4 - 44.90) | 18(12.9 - 23.1) |
| 60+ | 39.3(31.5 - 47.10) | 16.6(10.6 -22.5) |
| Total | 36.5(34.3 - 38.60) | 16.9(15.1 - 18.8) |
| Mariage status | ||
| Single | 17.9(12.4 - 23.40) | 5.3(2.1 - 8.6) |
| Married | 38.9(36.5 - 41.20) | 18.4(16.4 - 20.5) |
| Educational level | ||
| Illiterate | 37.3(30.2 - 44.30) | 17.7(12.5 - 22.9) |
| High school diploma or less | 37(34.4 - 39.60) | 18.1(15.8 - 20.4) |
| Associate degree | 33.7(29 - 38.40) | 13.9(10.3 - 17.4) |
| Masters degree or more | 43.8(25.4 - 62.10) | 3.1(-3.00 - 9.3) |
| Overweight | Obese | ||||
| Or (95%ci) | P-value | Or (95%ci) | <0.001 | ||
| Gender | Male/Female | 1.04 (0.80 - 1.35) | 0.795 | 1.98 (1.44 - 2.72) | |
| Age | 20-29 | 1 | 1 | <0.001 | |
| 30-39 | 1.75 (1.25 - 2.45) | <0.001 | 2.36 (1.50 - 3.72) | <0.001 | |
| 40-49 | 2.14 (1.55 - 2.96) | <0.001 | 3.59 (2.24 - 5.77) | 0.002 | |
| 50-59 | 1.60 (1.10 - 2.31) | 0.013 | 2.40 (1.37 - 4.20) | 0.017 | |
| 60+ | 1.70 (1.07 - 2.69) | 0.023 | 2.41 (1.17 - 4.96) | ||
| Educational level | Illiterate | 1 | 1 | 0.278 | |
| High school diploma or less | 1.20 (0.80 - 1.81) | 0.385 | 1.35 (0.78 - 2.32) | 0.337 | |
| Associate degree | 1.20 (0.76 - 1.91) | 0.436 | 1.36 (0.72 - 2.57) | 0.438 | |
| Masters degree or more | 1.58 (0.75 - 3.31) | 0.228 | 0.41 (0.04 - 3.85) | ||
| Marital status | Single | 1 | 1 | 0.002 | |
| Maried | 2.69 (1.73 - 4.20) | <0.001 | 3.24 (1.56 - 6.75) |
Discussion
In this study, we reported the prevalence of obesity and overweight by sex, marital status, and educational level in a population of Mashhad, as a representative of the Iranian population, according to the WHO criteria.
According to our results, 36.5% of the participants were overweight and 16.9% were obese. A review of the previous studies shows a lower prevalence of overweight and obesity in Mashhad when compared with Gorgan, Tehran, and Shiraz in both sexes while its prevalence was higher in Isfahan 14 15 16 17 18 . However, the prevalence of overweight and obesity in Mashhad is lower than the whole country; a national study that evaluated the BMI of Iranian men and women (BMI≤25) reported that the prevalence of overweight and obesity was 42.8% and 57% 19 . In 2008, the WHO reported a prevalence of 48.0% for overweight and 7.18% for obesity in the Middle East. A number of studies have reported a high prevalence of obesity and overweight in neighboring countries of Iran like the KSA, Turkey, and Oman but the prevalence is lower than countries like Italy, China, and Portugal 20 21 22 23 24 25 26 . These studies indicate that Iran, like its neighbors and as a developing country, is undertaking a socioeconomic transition; access to food and high calorie diets has increased in the past 10 years and physical activity has decreased due to the use of public and personal vehicles 27 . These changes, along with the prevalence of obesity, result in energy imbalance and increased burden of different diseases resulting from obesity; cardiovascular diseases are now the first cause of mortality and morbidity due to non-traumatic events in Iran 28 . However, the difference in the prevalence of obesity also depends on factors such as diet, access to food products, education level, and GDP. The prevalence of obesity and overweight is on the rise in Europe and America; According to a WHO report, the highest and lowest prevalence of obesity is observed in North America and Southeast Asia, respectively. In another study, Flegal et al. reported a prevalence of 68.8% for overweight and 35.7% for obesity in Americal population aged 20 years and over 29 . Concerns about the epidemic of obesity among the young generation are a major public health challenge because it increased the burden of the diseases incurs heavy costs on the society and increases the risk of atherosclerotic diseases and diabetes in the future. Therefore, preventive measures, increasing public awareness and knowledge, and physical activity are recommended to lower the prevalence of obesity. According to a study performed in a Japanese young population between 2003 and 2009, lifestyle modification decreased the prevalence of overweight and obesity 30 .
Our results showed that the prevalence of obesity and overweight was higher in women and men, respectively. These prevalence rates were higher than the finding of a national study that reported a prevalence of 11.1% for obesity in Iranian men 19 . Farhadian et al. also reported that the prevalence of obesity in men residing in Khorasan razavi Province was higher than other provinces 31. The results of the studies performed in Tehran, Golestan, Mazandaran, and Shiraz indicate the higher prevalence of obesity and overweight in women across the country 11 16 17 18 31 32 . There are also r eports of the rather high prevalence of overweight and obesity in women living in neighboring countries of Iran like Oman, Kuwait, and Turkey; for example, 62.65% of the women in Saudi Arabia suffer from overweight 20 21 22 23 . The reason could be that their lifestyle is similar to the lifestyle of Iranian women; most women in the Middle East are housewives and have little physical activity which is a major risk factor of obesity. In this regard, the prevalence of overweight and obesity is 4% and 10% lower respectively in Iranian female clerks that have more physical activity than their housewife counterparts 33 . There is anot he r reason to doubt the results of the above-mentioned studies. Most of these study collected information through census and door-to-door interview and as mentioned earlier, women spend most of their time at home in these countries and as a result, the information of the height and weight of other members of the household may not have been collected accurately. As mentioned in Results, the prevalence of obesity and overweight was higher in married versus single participants. A number of studies performed in Iran and other countries have confirmed the higher prevalence of Overweight in married people in both sexes 11 34 35 36 37 . The reason is not yet clear but cultural reasons like persuading the spouse to dine together or more attention to meals could be involved 16 .
It was mentioned earlier that the prevalence of overweight and obesity was lower in people with higher education (master’s degree and higher) versus people with lower education. Previous studies 26 31 38 39 40 h ave shown tha t people with higher education, in addition to having a correct insight and attitude toward the complications of obesity and observing an appropriate diet, have a higher income and spend money on appropriate foods more easily. The results of a cohort study on healthy women with normal BMI in England showed that they spent about 1000£ on buying high fiber, protein, and vitamin foods while the opposite was observed in people with a low income that spent most of their money on unhealthy fast foods containing high amounts of fat and carbohydrates, resulting in an increased risk of obesity 26 31 38 39 40 . However, anoth er study 37 re ported that people wit h an academic education are more prone to obesity because they mostly have office jobs and a sedentary lifestyle as compared to illiterate or low educated people who are mostly labors requiring a lot of energy.
Conclusions
According to the results of our study, the rising trend of the prevalence of overweight and obesity is concerning in the urban population of Mashhad. Due to the association of overweight and obesity with cardiovascular diseases and diabetes, it seems that more attention should be paid to obesity and overweight in Mashhad, which can be regarded as a necessity and a health system priority in Mashhad. For this reason, preventive measures like enhancing the socioeconomic status of the target population, increasing their awareness, and providing them with education on nutrition should be considered as the main objectives of health managers in this regard.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License (CC-BY 4.0) which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Ethics approval and consent to participate
Not to be applied.
Competing interests
The authors declare that they have no competing interests.
Funding
Not to be applied.
References
- Rivera Juan A, Barquera Simón, Campirano Fabricio, Campos Ismael, Safdie Margarita, Tovar Víctor. Epidemiological and nutritional transition in Mexico: rapid increase of non-communicable chronic diseases and obesity. Public health nutrition. 2002;5(1a):113-122. View Article PubMed Google Scholar
- Parkin D Max, Bray Freddie, Ferlay J, Pisani Paola. Global cancer statistics, 2002. CA: a cancer journal for clinicians. 2005;55(2):74-108. Google Scholar
- World Health organization (WHO, others Global Health Risks-Mortality and burden of disease attributable to selected major risks. Cancer. 2017;:. Google Scholar
- Fox Caroline S, Coady Sean, Sorlie Paul D, D’Agostino Ralph B, Pencina Michael J, Vasan Ramachandran S, Meigs James B, Levy Daniel, Savage Peter J. Increasing cardiovascular disease burden due to diabetes mellitus: the Framingham Heart Study. Circulation. 2007;115(12):1544-1550. View Article PubMed Google Scholar
- Johnson Mary Louise, Burke Bertha S, Mayer Jean. Relative importance of inactivity and overeating in the energy balance of obese high school girls. The American journal of clinical nutrition. 1956;4(1):37-44. Google Scholar
- Hubert Helen B, Feinleib Manning, McNamara Patricia M, Castelli William P. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study.. Circulation. 1983;67(5):968-977. Google Scholar
- Bell Janice F, Wilson Jeffrey S, Liu Gilbert C. Neighborhood greenness and 2-year changes in body mass index of children and youth. American journal of preventive medicine. 2008;35(6):547-553. Google Scholar
- Finucane Mariel M, Stevens Gretchen A, Cowan Melanie J, Danaei Goodarz, Lin John K, Paciorek Christopher J, Singh Gitanjali M, Gutierrez Hialy R, Lu Yuan, Bahalim Adil N, others National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9\textperiodcentered 1 million participants. The Lancet. 2011;377(9765):557-567. Google Scholar
- Flegal Katherine M, Carroll Margaret D, Ogden Cynthia L, Johnson Clifford L. Prevalence and trends in obesity among US adults, 1999-2000. Jama. 2002;288(14):1723-1727. Google Scholar
- Ng Marie, Fleming Tom, Robinson Margaret, Thomson Blake, Graetz Nicholas, Margono Christopher, Mullany Erin C, Biryukov Stan, Abbafati Cristiana, Abera Semaw Ferede, others Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. The lancet. 2014;384(9945):766-781. Google Scholar
- Hajian-Tilaki KO, Heidari B. Prevalence of obesity, central obesity and the associated factors in urban population aged 20-70 years, in the north of Iran: a population-based study and regression approach. Obesity reviews. 2007;8(1):3-10. Google Scholar
- Azadbakht Leila, Esmaillzadeh Ahmad. Dietary and non-dietary determinants of central adiposity among Tehrani women. Public health nutrition. 2008;11(5):528-534. Google Scholar
- Azadbakht Mirmiran Shiva Azizi General obesity and central adiposity in a representative sample of Tehranian adults: prevalence and determinants. International journal for vitamin and nutrition research. 2005;75(4):297-304. Google Scholar
- Rashidy-Pour A, Malek M, Eskandarian R, Ghorbani R. Obesity in the Iranian population. Obesity reviews. 2009;10(1):2-6. Google Scholar
- Veghari Gholamreza, Sedaghat Mehdi, Joshghani Hamidraza, Banihashem Samieh, Moharloei Pooneh, Angizeh Abdolhamid, Tazik Ebrahim, Moghaddami Abbas. Obesity and risk of hypercholesterolemia in Iranian northern adults. ARYA atherosclerosis. 2013;9(1):2. Google Scholar
- Moghimi-Dehkordi B, Safaee A, Vahedi M, Pourhoseingholi A, Pourhoseingholi MA, Ashtari S, Zali MR. Overweight and obesity and related factors in urban Iranian population aged between 20 to 84 years. Annals of medical and health sciences research. 2013;3(2):171-176. Google Scholar
- Ayatollahi SMT, Ghoreshizadeh Z. Prevalence of obesity and overweight among adults in Iran. Obesity reviews. 2010;11(5):335-337. Google Scholar
- Âghdak P, others Survey of obesity, underweight and associated factors in elderly people, using some of anthropometric indices in Isfahan City, 2004. Journal of Mazandaran University of Medical Sciences. 2006;16(52):117-125. Google Scholar
- Janghorbani Mohsen, Amini Masoud, Willett Walter C, Gouya Mohammad Mehdi, Delavari Alireza, Alikhani Siamak, Mahdavi Alireza. First nationwide survey of prevalence of overweight, underweight, and abdominal obesity in Iranian adults. Obesity. 2007;15(11):2797-2808. Google Scholar
- Al-Lawati Jawad A, Jousilahti Pekka J. Prevalence and 10-year secular trend of obesity in Oman.. Saudi medical journal. 2004;25(3):346-351. Google Scholar
- Alsaif Mohammed A, Hakim Iman A, Harris Robin B, Alduwaihy Mansour, Al-Rubeaan Khalid, Al-Nuaim Abdul Rahman, Al-Attas Omar S. Prevalence and risk factors of obesity and overweight in adult Saudi population. Nutrition Research. 2002;22(11):1243-1252. Google Scholar
- Musaiger Abdulrahman O, Al-Mannai Mariam, Tayyem Reema, Al-Lalla Osama, Ali Essa YH, Kalam Faiza, Benhamed Mofida M, Saghir Sabri, Halahleh Ismail, Djoudi Zahra, others Prevalence of overweight and obesity among adolescents in seven Arab countries: a cross-cultural study. Journal of obesity. 2012;2012:. Google Scholar
- Yumuk Volkan D, Hatemi Husrev, Tarakci Tunc, Uyar Nurettin, Turan Nurten, Bagr\iacik Nazif, Ipbuker Ali. High prevalence of obesity and diabetes mellitus in Konya, a central Anatolian city in Turkey. Diabetes research and clinical practice. 2005;70(2):151-158. Google Scholar
- Micciolo Rocco, Di Francesco Vincenzo, Fantin Francesco, Canal Luisa, Harris Tamara B, Bosello Ottavio, Zamboni Mauro. Prevalence of overweight and obesity in Italy (2001-2008): is there a rising obesity epidemic?. Annals of epidemiology. 2010;20(4):258-264. Google Scholar
- Tian Huiguang, Xie Hongxiang, Song Guide, Zhang Hong, Hu Gang. Prevalence of overweight and obesity among 2.6 million rural Chinese adults. Preventive medicine. 2009;48(1):59-63. Google Scholar
- Santos A-C, Barros H. Prevalence and determinants of obesity in an urban sample of Portuguese adults. Public health. 2003;117(6):430-437. Google Scholar
- Ghassemi Hossein, Harrison Gail, Mohammad Kazem. An accelerated nutrition transition in Iran. Public health nutrition. 2002;5(1a):149-155. Google Scholar
- Shab-Bidar S, Hosseini-Esfahani F, Mirmiran P, Hosseinpour-Niazi S, Azizi F. Metabolic syndrome profiles, obesity measures and intake of dietary fatty acids in adults: Tehran Lipid and Glucose Study. Journal of human nutrition and dietetics. 2014;27(s2):98-108. Google Scholar
- Flegal Katherine M, Carroll Margaret D, Kit Brian K, Ogden Cynthia L. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010. Jama. 2012;307(5):491-497. Google Scholar
- Kurokawa Naoyuki, Satoh Hiroshi. Recent trends of body mass index distribution among school children in Sendai, Japan: Decrease of the prevalence of overweight and obesity, 2003-2009. Obesity research & clinical practice. 2011;5(1):e1-e8. Google Scholar
- Farhadian Maryam, Moghimbeigi Abbas, Aliabadi Mohsen. Mapping the obesity in iran by bayesian spatial model. Iranian journal of public health. 2013;42(6):581. Google Scholar
- Bahrami Hossein, Sadatsafavi Mohsen, Pourshams Akram, Kamangar Farin, Nouraei Mehdi, Semnani Shahriar, Brennan Paul, Boffetta Paolo, Malekzadeh Reza. Obesity and hypertension in an Iranian cohort study; Iranian women experience higher rates of obesity and hypertension than American women. BMC public health. 2006;6(1):158. Google Scholar
- Navadeh S, Sajadi L, Mirzazadeh A, Asgari F, Haghazali M. Housewives’ obesity determinant factors in iran; national survey-stepwise approach to surveillance. Iranian journal of public health. 2011;40(2):87. Google Scholar
- Dinour Lauren, Leung May May, Tripicchio Gina, Khan Sahar, Yeh Ming-Chin. The association between marital transitions, body mass index, and weight: a review of the literature. Journal of obesity. 2012;2012:. Google Scholar
- Mullan Harris Kathleen, Lee Hedwig, DeLeone Felicia Yang. Marriage and health in the transition to adulthood: Evidence for African Americans in the Add Health Study. Journal of Family Issues. 2010;31(8):1106-1143. Google Scholar
- Umberson Debra, Liu Hui, Powers Daniel. Marital status, marital transitions, and body weight. Journal of Health and Social Behavior. 2009;50(3):327-343. Google Scholar
- Laurier Dominique, Guiguet Marguerite, Chau Nguyen Phong, Wells James A, Valleron Alain-Jacques. Prevalence of obesity: a comparative survey in France, the United Kingdom and the United States.. International journal of obesity and related metabolic disorders: journal of the International Association for the Study of Obesity. 1992;16(8):565-572. Google Scholar
- Gutiérrez-Fisac Juan L, Regidor Enrique, Rodríguez Carmen. Trends in obesity differences by educational level in Spain. Journal of Clinical Epidemiology. 1996;49(3):351-354. Google Scholar
- Cade Janet, Upmeier Hendrike, Calvert Claire, Greenwood Darren. Costs of a healthy diet: analysis from the UK Women's Cohort Study. Public health nutrition. 1999;2(4):505-512. Google Scholar
- Dayan Y Bar, Elishkevits K, Grotto I, Goldstein L, Goldberg A, Shvarts S, Levin A, Ohana N, Onn E, Levi Y. The prevalence of obesity and associated morbidity among 17-year-old Israeli conscripts. Public Health. 2005;119(5):385-389. Google Scholar