Open Access
Open Access Abstract
Background: Mercury is used by artisanal — small-scale (ASM) gold miners throughout the World. In 2014, the Sudanese government produced over 60 tons of gold, which make Sudan ranked Africa's third-largest gold miner. Also, Sudan is ranked the 15th global producer. In 2015, over 1 million miners participated in gold mining and extraction. Objective: This study aimed to determine mercury health risk in Sudanese traditional gold mining activities area.
Method: This is an analytical cross-sectional observational stud. The studied population was from ALTWAHEN near ABUHAMED. Urine analysis was supported by epidemiological questionnaires designed by (EPI INFO software) following WHO guidelines. Eighty-six respondents completed the questionnaire. The mercury level was determined in 58 urine sample by Petroleum Laboratories Using Direct Mercury Analyzer DMA- 80 instrument. The epidemiological data were analyzed by (EPI INFO).
Result: 98% exceed concentration of 100 ug/L which contaminated concentration for occasionally exposed, mean urinary mercury concentration 2785 ug/L, the highest mercury concentration worldwide reported by our study 10250 ug/L, Symptoms in 58 patient showed as Problem finding correct word 46.6%, memory problem 27.6%, problem with thinking clearly 29.3%, nervousness 31%, sadness 46.5%, sexual problem 36.2%, headache 51.7%, excessive salivation 43%, drowsy 48.3%.
Conclusion: In this study, the highest urinary mercury concentration was reported (10250 ug/L) compared to other studies. Mercury concentration with no significant difference between the miner groups and others. Also, this study found high incidents of neurological symptoms associated with neurotoxicity. The problem with thinking significantly correlated to the age weighted by mercury concentration. Only tremor significantly related to the time living in the mining area. Otherwise, no significant relationship between mercury concentration ,symptoms and time living in the area.
Recommendation: conducting Interventional study by using chelation therapy, Gold miners should use safety tools, Activation of laws and conventions (MINAMATA convention).
Introduction
The first mining boom episode in Sudan gold, iron ore and copper mining activities in Nubia since 3000-1500 BC. In 2015, over 1 million miners participated in gold mining and extraction, with 4 million family dependents benefited from mined gold revenues. The traditional gold mining activities cover 14 of the 18 Sudanese states. In 2014, the government produced over 60 tons of gold, which maked Sudan ranked Africa's third-largest gold miner, and pushed it into the top 15 global producers 1 , 2 , 3 .
Mercury is used by artisanal and small-scale (ASM) gold miners throughout the World 4 , 5 . The heavy metals cadmium, lead, and mercury are common air pollutants emitted mainly as a result of various industrial activities.
It exists in the environment in three forms: elemental mercury (poisonous as vapor), organic mercury (methyl mercury and ethyl mercury), and inorganic mercury (mercuric mercury). All these forms have toxic health effects 6 .
Mercury vapor can elicit the nephrotic syndrome, characterized by excessive loss of protein (mainly albumin) in the urine, and edema 7 , 8 .
Rationale and Objectives
Rationale
Traditional gold mining using mercury to form gold amalgam is widely used in South America, Africa, and Asia. Many studies have investigated the health risk due to mercury exposure worldwide and determined health effect due to mercury exposure. In Sudan, the gold mining activities are spread. However, there is only a few studies covering this area. So, we conduct this research.
Objective
General objective
To investigate mercury health risk in Sudanese traditional gold mining activities.
Specific objective
To detect mercury exposure among miners and other non-miners
To observe the general toxicity among the gold mining worker
To observe the health effect of mercury in gold mining worker
To observe the neurotoxicity in gold mining worker
To measure the concentration of mercury in urine among gold mining worker
Methods
Study Design
An analytical cross-sectional observational study.
Study Area
The study was carried in Altwahen gold mining area, located 12 km from Abuhamad city, in Nile river state-Sudan.
Study Population
All participants are from Altwahen gold mining area included gold miners who worked in Altwahen and non-miners.
Inclusion Criteria
The study included all participant who completed the questionnaire and gave urine samples (N=58).
Exclusion Criteria
The study excluded participants who had neurological diseases, current malaria, current injuries from accidents, and participant who did not provide urine samples (N=27).
Sample size
The sample size calculated as 10% (85) of the population approximately (850).
Material and methods
The urine samples were collected in four 50-mL plastic containers. The analysis was done in laboratories by using Direct Mercury Analyzer DMA-80 instrument.
Data collection
The questionnaire was designed as WHO guideline using EPI INFO software. Interview questionnaire was conducted with all the participants. Data were collected, analyzed, and tabulated.
Data analysis
Data analysis and presentation by the EPI INFO software and Excel program.
Ethical considerations
Ethical documents were obtained from Omdurman Islamic university ethical committee.
Results
In this study a total number of 58 participants were evaluated during the data collection period. After being properly revised, data were classified and presented in tables as:
Distribution According To Personal Data (N = 58)
Sixty two percent of the study participants were miners. However, 55% of participants were single considering that almost 7% of our study populations were children's under 18 years old working in the field, 58.6% between (19-27 years old) Table 1 .
| Parameter | N (%) |
| Marital Status | |
| Single | 32 (55.17%) |
| Married | 26 (44.83 %) |
| Age | |
| 10 - 18 | 4(6.90%) |
| 19 -27 | 34(58.62%) |
| 28 -35 | 12(20.69%) |
| 36 - 43 | 4(6.90%) |
| 44 -51 | 2(3.45%) |
| 52 -59 | 2(3.45%) |
| Job description | |
| Miner | 36 (62.07%) |
| Well Drilling Worker | 4(6.90%) |
| Others | 18(31.03%) |
To detect the mercury exposure among miners and other non-miners
65.5% of study participants has history of working as miner with mercury contact. On the other hand, 50% reported work as the place of stored mercury containers and 46.6% never store mercury Table 2 .
| Question/Response | N(%) |
| History Of Working As Miner With Mercury Contact | |
| No | 20 (34.48%) |
| Yes | 38 (65.52%) |
| Place of Stored Mercury container | |
| Home | 2 (3.4%) |
| work | 29 (50%) |
| Never store mercury | 27 (46.6) |
To observe the health effect of mercury in gold mining worker
When we questioned participant about the health effect as a result of mercury exposure, feeling Weakness reported only by 29% and, Feel Sleepy or Drowsy reported by 48.2%. On the contrary, 69% never experience palpitation, 96.5% never experienced any chronic disease or diabetes Table 3 .
| Question/Response | N(%) |
| Feeling Weakness | |
| Same As Usual | 41(70.69%) |
| Worse Than Usual | 8(13.79%) |
| Much Worse Than Usual | 9(15.52%) |
| Feel Sleepy Or Drowsy | |
| Same As Usual | 30(51.72%) |
| More Than Usual | 18(31.03%) |
| Much Worse Than Usual | 10(17.24%) |
| Palpitation | |
| Never | 40(68.97%) |
| At Least Once A Day | 5(8.62%) |
| At Least Once A Week | 10(17.24%) |
| At Least Once A Month | 3(5.17%) |
| No | 56(96.55%) |
| Yes | 2(3.45%) |
| No | 56(96.55%) |
| Yes | 2(3.45%) |
Distribution according to general health (N = 58)
In miner and none miner general health problems and other symptoms, in miners metallic taste and palpitation reported by 33% -36% respectively, while well drillers never experienced palpitation and only 16.6% had metallic taste. However, respiratory allergy and cough in miners reported by 27.7% and %52.7% respectively, among all participants 60% reported appetite problems while sexual problems and excessive salivation reported by 36% and 43% respectively Table 4 .
| Symptoms | Miners N=36 (%) | Well Drilling N= 6 (%) | Others N=16 (%) | All N=58 (%) |
| Metallic Taste | 12 (33.33) | 1(16.6) | 5(31.25) | 31% |
| Palpitation | 13(36.1) | 0(0.00) | 5(31.25) | 31% |
| Feel Week | 14(38.88) | 1(16.66) | 3(18.75) | 31% |
| Respiratory Allergy | 10(27.77) | 1(16.66) | 2(12.50) | 22.4% |
| Cough | 19(52.77) | 2(33.33) | 6(37.50) | 46.5% |
| Nausea | 8(22.22) | 2(33.33) | 2(12.50) | 20.7% |
| Gingivitis | 4(11.11) | 0(0.00) | 0(0.00) | 6.9% |
| Excessive Salivation | 20(55.55) | 1(16.66) | 4(25.00) | 43% |
| Appetite Problem | 22(61.11) | 2(33.33) | 11(68.75) | 60% |
| Sexual Problem | 12(33.33) | 3(50.00) | 6(37.50) | 36.2 |
Distribution According To Neuropsychological Status
Headache was reported by 51.7% of the study participants, among all our participants 46.5% experience problem finding correct ward and feeling sad. On the other hand, nervousness reported by 31% and 19% had sleeping problems Table 4 , Table 5 , Table 6 .
| Symptoms | Miners N=36 (%) | Well Drilling N= 6 (%) | Others N=16 (%) | All N=58 (%) |
| Feel Prickling Aching | 2(5.5) | 0(0.00) | 0(0.00) | 3.4% |
| Drowsy | 18(50.00) | 2(33.33) | 8(50.00) | 48.3% |
| Headache | 20(55.55) | 7(116.6) | 3(18.75) | 51.7% |
| Problem With Eye Strain | 4(11.11) | 0(0.00) | 1(6.25) | 8.6% |
| Tremor | 15(41.66) | 2(33.33) | 5(31.25) | 38% |
| Symptoms | Miners N=36 (%) | Well Drilling N= 6 (%) | Others N=16 (%) | All N=58 (%) |
| Nervousness | 10(27.7) | 2 (33.3) | 6(37.5) | 31% |
| Feeling Sad | 19(52.77) | 2(33.33) | 7(43.75) | 46.5% |
| Problem With Thinking Clearly | 13(36.11) | 1(16.66) | 3(18.75) | 29.3% |
| Problem Finding Correct Ward | 20(55.55) | 2(33.33) | 5(31.25) | 46.6% |
| Memory Problem | 10(27.77) | 1(16.66) | 5(31.25) | 27.6% |
| Sleep Problem | 6(16.66) | 2(33.33) | 3(18.75) | 19% |
Distribution according to concentration of mercury in urine among gold mining worker
Mean mercury concentration (ppb) for well drilling was 2902.73 and 3241.49 for others compared to 2563.17 for miners and among the miners the highest was 2795.85 for washers Table 7 , Table 8 , Table 9 .
| Concentration from 3.1 to 501 ppb | Concentration from 610 to 1295 ppb | Concentration from 1452 to 2685 ppb | Concentration from 3173 to 5708 ppb | Concentration from 5744 to 10250 ppb |
| 3.18 | 610.7 | 1452 | 3173 | 5744 |
| 206.2 | 660.4 | 1556 | 3252 | 5829 |
| 262.7 | 757.6 | 1622 | 3529 | 5852 |
| 276.2 | 777.8 | 1764 | 3639 | 6367 |
| 281.1 | 808.7 | 1964 | 3770 | 6453 |
| 307.9 | 896.7 | 2028 | 3858 | 6862 |
| 350.3 | 1055 | 2165 | 3932 | 6995 |
| 481.8 | 1055 | 2329 | 4123 | 7598 |
| 494.8 | 1098 | 2380 | 5010 | 10030 |
| 501.5 | 1135 | 2428 | 5372 | 10250 |
| 1142 | 2498 | 5708 | ||
| 1148 | 2498 | |||
| 1234 | 2685 | |||
| 1295 |
| Job Description | Frequency | Mean Mercury Concentration (ppb) |
| Miner | 36 | 2563.17 |
| Well Drilling Worker | 6 | 2902.73 |
| Others | 16 | 3241.49 |
| Total | 58 | 2785.4238 |
| Miner group | Mean mercury concentration (ppb) | Minimum (ppb) - Maximum (ppb) |
| Gold Refiner | 2180.80 | 206.2 - 3252 |
| Gold Shop Worker | 1994.65 | 350.3 - 1994.65 |
| Miller | 2076.88 | 276.2 - 3932 |
| Washer | 2795.85 | 3.1 - 3471.5 |
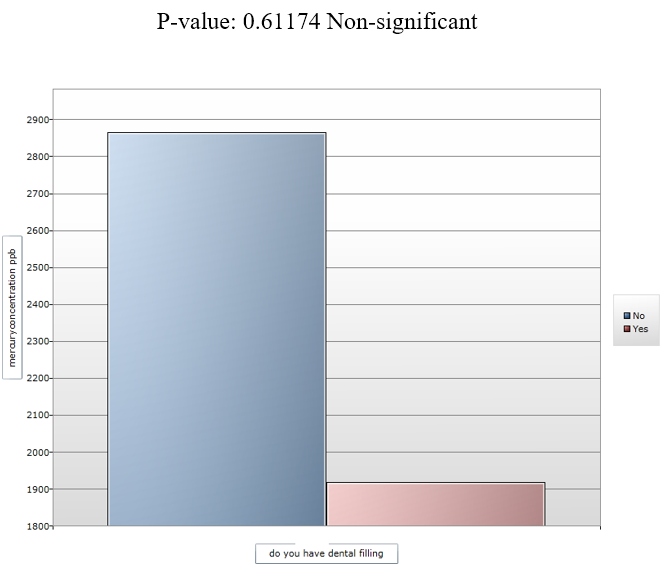
Figure 2 . Tremor symptoms cross tabulated by time living in mining area (days).



| Obs | Total | Mean | Variance | Std Dev |
| 37540.1000 | 897014.0000 | 23.8948 | 141609.5922 | 376.3105 |
| 102409.4780 | 3257274.3500 | 31.8064 | 372216.9115 | 610.0958 |
| 21605.0000 | 461141.0000 | 21.3442 | 52414.1701 | 228.9414 |
Discussion
In our study, the miners and others in the mining area urine sample analysis showed very high mercury level (approximately 98 %) exceed the concentration of 100 ppb which is the contaminated concentration for occasionally exposed.
Rosa et al. detected the mercury level in urine in 22% of the workers in gold shops in Brazil(Hg < 50 ppm 9 ) while in this research 100% the gold shop worker contaminated by mercury with the mean mercury concentration of 1994.6500 ppb. These gold shop worker stored mercury in their shops, and they continuously smell mercury vapor in their shops.
However, in this research in the mining area, there were non-miner workers such as coffee boys, merchants, and tailors, etc . They represent 31% of our research participants with the mean urinary mercury level for non-miners was 3241.49 ppb which is an extremely high value compared to occasional exposure or non-exposure according to the guidelines. Oosthuizen et al. studied in South Africa and found 14 (50%) of the urine samples exceeded the guideline for mercury in urine (<5.0 μg/g creatinine) for those not exposed occasionally 10 . The authors concluded that some individuals might be occasionally exposed to mercury through small-scale gold mining activities. The non-miners in our study were exposed to mercury due to their work in the contaminated area in the mining work place.
The gold refiner in our study have the mean urinary mercury level of 2180.80 μg/l as Hurtado J. 11 defined them in a term of “smelter”. The high level of mercury is because they small the vapor of mercury in their regular job.
Hurtado et al. in a study in Peru 11 , found high levels (mean 728 μg/L) of mercury in the urine of those directly involved in smelting (N=6), compared to the controls (4 μg/L). The mean level of mercury in urine for all participant in our study was 2785.4238 ppb, N =(58) which is a unique finding because it was the highest urinary mercury level reported. On the other hand, in Tanzania 12 , urinary mercury concentrations found in 36% of individuals (N=45) involved in amalgamation were between 50 and 100 μg/g creatinine, with four samples >100 μg/g creatinine. The mean mercury level in control urine samples was 5 µg/g creatinine.
This study is one of a few studies in Sudan aimed to evaluate the mercury toxicity among Sudanese people. Tayrab et al . 13 , conducted a study in Abu Hamad and found a significant increase in serum mercury levels in the gold miners N, serum mercury level (1.40 ± 0.94 μg/L)). In our study, we agree that there is a significant increase in biological parameter urinate mercury level. We also found that 20% of our participants had a respiratory allergy, 72% of these cases were due to dust and smelling of mercury vapor. One of our findings was that 15% of those have productive cough (N 26) mentioned they have bloody color sputum. This is very important because the color of ores is red. So, that is the color of inhaled dust, not blood 14 .
Tayrab et al . concluded that forced expiratory volume in the first second (FEV1) and forced vital capacity (FVC) decreased but with no statistical significance 13 .
The washers in our study were those were involved in washing the ores with mercury. They contacted with mercury topically with their hands. We found the mean urinary mercury level of the washer was 2795.85 ppm (N 24). The mercury level of the washer was significantly higher compared to the values reported by Hursh et al . 15 . Hursh et al. concluded that dermal absorption of elemental mercury is limited by estimating that dermal absorption only contributed approximately 2.6% of the absorbed mercury following exposure to elemental mercury vapor in the air; the other 97.4% occurred through inhalation 15 .
The result of this study showed no significant relationship between amalgam filing and mercury concentration, which is the same as Hursh et al . 15 that there is no relationship between mercury concentrations in lower parts of the brain and the number of amalgam fillings in the mouth.
This result showed significantly high mercury level in urine although Afnan Abuyazed in her research 16 Mercury Pollution from Artisanal Gold Mining Activities in Abo Hamad Sudan showed that mercury concentration in Sudanese hair of gold mining worker was significant. In this research, the unique urinary mercury level with the mean 2785.4238 ppb was due to the use of urinary mercury as the biological monitor. Clarkson et al. found that urine and feces are the main excretory pathways of elemental mercury and inorganic mercury compounds in humans, with an absorbed dose half-life of approximately 1–2 months) 17 . After a short-term high-level mercury exposure in humans, urinary excretion accounts for 13% of the total body burden. After long-term exposure, urinary excretion increases to 58%.
In this study, mercury poisoning symptoms was found in 46.6% of the participants including memory problem (27.6%), problem with thinking clearly (29.3%), nervousness (31%), sadness (46.5%), sexual problem (36.2%), headache (51.7%), excessive salivation (43%), drowsy (48.3%). These results showed no correlation between symptoms and urinary concentration, however one of our research limitations was the feasibility to investigate the renal toxicity. However, neurological symptoms and neuropsychological and other symptoms are present in high percentage tremor but with no significant correlation with the concentration of mercury in urine.
Aks et al . found that there was no correlation between symptoms and urinary and blood concentration of mercury 18 , which supports our findings. This observation may be related to other co-founding factors.
One of our unique findings was that the tremor was significantly associated with the staying time in the mining area (p = 0.0136). Although there is no significant correlation between the symptoms and the concentration of mercury in urine, the time of living in the mining area is one of important co-founders suggested by our study.
In this research, there was no significant relation between the concentration of mercury and the time of living in the mining area, which may be justified because of the toxicodynamic properties of mercury that there is a difference in elimination rate of mercury over time. In the literatures, Clarkson et al. found that the urine and feces are the main excretory pathways of elemental mercury and inorganic mercury compounds in humans, with an absorbed dose half-life of approximately 1–2 months 17 . After a short-term high-level mercury exposure in humans, urinary excretion accounted for 13% of the total body burden. After long-term exposure, urinary excretion increases to 58%.
In the epidemiological questionnaire, approximately 40% (N = 36) of the responders reported that they experienced hand tremor. Fawer et al . 19 also concluded that tremor was greater in the exposed group than in controls ( P < 0.001) and was significantly related to the duration of exposure and age. We found a significant relationship between tremor a and duration of exposure but the age had no significant contribution to our research.
The neurotoxicity of mercury from occasional exposure is well-known. Ehrenberg et al . 20 , mentioned that there is a significant effect on tremor or cognitive skills or other central nervous system effects among groups exposed occasionally to similar or slightly higher levels of mercury. Tremor, abnormal Romberg test, dysdiadochokinesis, and difficulty with heel-to-toe gait were also observed in thermometer plant workers.
In the epidemiological questionnaire, the result showed 5.5% of miners felt prickling aching, others non-miner had no such symptoms. This is may be due to miners being in direct contact with mercury. 50% of miners felt drowsy, and 50% of others non-miner felt drowsy, which might be a sign of air pollution in the area. Our result showed 51% of participants had headache, and 29% reported the problem in thinking clearly, 64.5% reported the problem in finding correct ward while 20% of this group reported it was much worse than usual. All these signs suggested that Sudanese gold mining had neurotoxicity signs due to contamination of the mining area. 27% (N 58) had memory problem. Our results showed in table 3.5.2 the age and problem with thinking clearly had a very a significant result weighted to mercury concentration p-value (0.006). Children at school age in the minidng area are at risk of decreased cognitive function.
Meyer-Baron et al . 21 conducted a review of 18 epidemiological studies dealing with occupational exposure to inorganic mercury in workers with mean levels of internal exposures in the range 3–192 μg/g creatinine showed associations with attention, memory, motor performance and exposure, although the quantitative dose-response relationships could not be established.
Regarding neurobehavioral effects, this study reported that 48% of the participants (N = 58) feeling sad, 31% (N = 58) feeling nervous neurobehavioral effects, increasing hostility and anxiety levels, and decreasing mental stability and inferiority complex. The neurobehavioral effect of mercury in mining area may be realted to the violence rate in the mining area. A limitation of our research is there was no accessibility to evaluate renal toxicity. However, recently, a WHO review concluded, on the basis of existing studies, that adverse effects on the kidney usually occur at exposures higher than those that induce neuro-physiological effects. There is a scientific gap in human’s lowest harmful or non-adverse exposure levels, especially for long-term exposure. The result of this study showed high neuro-physiological symptoms. However, the effect of mercury on the renal system was not evaluated.
This result documented the highest level worldwide mercury concentration which indicates chronic toxicity. Although the study evaluated the health effect of gold mining worker, we could predict the environmental pollution by employing the regression line determined by 22 , 23 , a urinary level of 2785.4ppb could be calculated to estimate the airborne mercury concentration. By using personal breathing zone mercury measurements, it was estimated that in continuous 8 h/day occupational exposure, an airborne mercury concentration of 1 mg/m3 leads to an average urinary mercury concentration of 1.4 mg (7 μmol)/liter (variation between individual studies, 0.7–2.3 mg [3.5–11.5 μmol]/liter (82).
Studies conducted by Lindstedt et al . 23 , reported a correlation between airborne mercury and mercury in blood and urine. However, results are not consistent across studies. Also, it is unknown whether the ratio between concentrations in urine and blood is constant at different exposure levels.
This study showed that the Hugh level of mercury in urine sample taken from Altwahen area 12 km away from Abou Hamad in Nile river state (Sudan) (mean 2785.4238 ppm) and tremor 37%, which is different from the research done by global mercury project 13 . The study showed that the population's exposure did not lead to high mercury levels in blood, hair, or urine. The only symptom of chronic mercury intoxication observed were standing tremors and eyelids, lips, tremors in 40% of participants. The study found that it was not possible to demonstrate that there was any relationship between these signs and mercury use or mercury levels in the blood, urine or hair sample.
This difference between our findings and the global mercury project result may be due to differences in many factors including research methodology, geographical area location, amount of mercury use, and workplace method. Baeuml et al . 24 reported mercury levels also differ considerably between countries, which reflects a diverse background burden due to different fish eating habits and different workplace methods.
Conclusions
The aim of the study was to test mercury poisoning in small gold mining activity at Abo- Hamad city in Al-Tawahean area. We found that the mean of mercury concentration in urine was 2785 ppb, which indicated a high toxicity level. The highest mercury concentration reported by this research was 10250 ppb with no significant difference between miner groups and others. Also, we found high incidents of neurological symptoms associated with neurotoxicity.
Problem with thinking clearly has significant correlation to age weighted by mercury concentration. Tremor is definitely related to the time living in the mining area. Otherwise, there was no significant relationship between mercury concentration, symptoms and time living in the area.
Recommendation
Interventional study should be done using chelating therapy. Renal toxicity should be evaluated in people living in gold mining areas. Gold miners should use safety tolls (gloves, mask, etc .). Monitoring the environment and organic mercury in water. Working time in the mining area should be adjusted. Studies at Abo-hamad city should be conducted to evaluate the community exposure to mercury including pregnant women and children at school age. Toxicological study should be conducted to measure mercury in Nile river fish. Alternative technologies should be implemented to reduce mercury emission.
Competing Interests
Authors have no conflict of interest.
Authors' Contributions
Conceptualization of work & its realization was done by Dr.Salah Altag, all authors participate in acquisition of data, analysis and interpretation of data; The correspondent author Dr.Lina and Dr.Hind participate in drafting the article or revising it critically for important intellectual content; All authors give final approval of the version to be submitted and any revised version.
References
- Sudan Central Bank of. Annual Reports 2002-2014. . ;:. Google Scholar
- Co Report on Artisanal Mining Impacts prepared for Ministry of Finance 2015. . ;:. Google Scholar
- Minerals Ministry of. Reports 2014-2015. . ;:. Google Scholar
- Taylor H., Appleton J.D., Lister R., Smith B., Chitamweba D., Mkumbo O.. Environmental assessment of mercury contamination from the Rwamagasa artisanal gold mining centre, Geita District, Tanzania. Sci Total Environ. 2005;343(1-3):111-33. View Article PubMed Google Scholar
- Santa Rosa R., Müller R.C., Alves C.N., Sarkis J.E., Bentes M.H., Brabo E., others Determination of total mercury in workers' urine in gold shops of Itaituba, Pará State, Brazil. Sci Total Environ. 2000;261(1-3):169-76. View Article PubMed Google Scholar
- Ibrahim D., Froberg B., Wolf A., Rusyniak D.E.. Heavy metal poisoning: clinical presentations and pathophysiology. Clin Lab Med. 2006;26(1):67-97. View Article PubMed Google Scholar
- World Health Organization. Air quality guidelines for Europe. WHO Reg Publ Eur Ser. 2000;:V-X. Google Scholar
- Santa Rosa R., Müller R.C., Alves C.N., Sarkis J.E., Bentes M.H., Brabo E., others Determination of total mercury in workers' urine in gold shops of Itaituba, Pará State, Brazil. Sci Total Environ. 2000;261(1-3):169-76. View Article PubMed Google Scholar
- Santa Rosa R., Müller R.C., Alves C.N., Sarkis J.E., Bentes M.H., Brabo E., others Determination of total mercury in workers' urine in gold shops of Itaituba, Pará State, Brazil. Sci Total Environ. 2000;261(1-3):169-76. View Article PubMed Google Scholar
- Oosthuizen M.A., John J., Somerset V.. Mercury exposure in a low-income community in South Africa. S Afr Med J. 2010;100(6):366-71. View Article PubMed Google Scholar
- Hurtado J., Gonzales G.F., Steenland K.. Mercury exposures in informal gold miners and relatives in southern Peru. Int J Occup Environ Health. 2013;:. Google Scholar
- van Straaten P.. Human exposure to mercury due to small scale gold mining in northern Tanzania. Sci Total Environ. 2000;259(1-3):45-53. View Article PubMed Google Scholar
- Tayrab Eltayeb, Elrahim Manahil Azhary Abd, Elameen Mohammed Elbagir Ali, Yassin Ahmed, Kodi Ali. Human Mercury Exposure Associated with Artisanal Gold Miners in Sudan. Int J Earth Environ Sci. 2016;1(118):. View Article Google Scholar
- Kudsk F.N.. The influence of ethyl alcohol on the absorption of mercury vapour from the lungs in man. Acta Pharmacol Toxicol (Copenh). 1965;23(2):263-74. View Article PubMed Google Scholar
- Hursh J.B., Cherian M.G., Clarkson T.W., Vostal J.J., Mallie R.V.. Clearance of mercury (HG-197, HG-203) vapor inhaled by human subjects. Arch Environ Health. 1976;31(6):302-9. View Article PubMed Google Scholar
- A.A. Mohamed, Koveke E.P., Ohira S.-I., Toda K.. Mercury Pollution from Artisanal Gold Mining Activities in Sudan. . 2015;:062-064. Google Scholar
- Clarkson T.W., Magos L., Cox C., Greenwood M.R., Amin-Zaki L., Majeed M.A.. Tests of efficacy of antidotes for removal of methylmercury in human poisoning during the Iraq outbreak. J Pharmacol Exp Ther. 1981;218(1):74-83. PubMed Google Scholar
- Aks S.E., Erickson T., Branches F.J., Naleway C., Chou H.N., Levy P., others Fractional mercury levels in Brazilian gold refiners and miners. J Toxicol Clin Toxicol. 1995;33(1):1-10. View Article PubMed Google Scholar
- Fawer R.F., de Ribaupierre Y., Guillemin M.P., Berode M., Lob M.. Measurement of hand tremor induced by industrial exposure to metallic mercury. Br J Ind Med. 1983;40(2):204-8. View Article PubMed Google Scholar
- Ehrenberg R.L., Vogt R.L., Smith A.B., Brondum J., Brightwell W.S., Hudson P.J.. Effects of elemental mercury exposure at a thermometer plant. Am J Ind Med. 1991;19(4):495-507. View Article PubMed Google Scholar
- Meyer-Baron M., Schaeper M., Seeber A.. A meta-analysis for neurobehavioural results due to occupational mercury exposure. Arch Toxicol. 2002;76(3):127-36. View Article PubMed Google Scholar
- Roels H., Abdeladim S., Ceulemans E., Lauwerys R.. Relationships between the concentrations of mercury in air and in blood or urine in workers exposed to mercury vapour. Ann Occup Hyg. 1987;31(2):135-45. PubMed Google Scholar
- Lindstedt G., I I. Gottberg, Holmgren B., Jonsson T., Karlsson G.. Individual mercury exposure of chloralkali workers and its relation to blood and urinary mercury levels. Scand J Work Environ Health. 1979;5(1):59-69. View Article Google Scholar
- Baeuml J., Bose-O'Reilly S., Gothe R.M., Lettmeier B., Roider G., Drasch G.. Human biomonitoring data from mercury exposed miners in six artisanal small-scale gold mining areas in Asia and Africa. Minerals (Basel). 2011;1(1):122-43. View Article Google Scholar