Open Access
Open Access Abstract
The end of the first quarter of the 21st century will be known as when there was a deadly pandemic due to COVID-19 infection. The four subfamilies of a, b , â–³, g have a genetic variation ranging between 26 to 32 kb. Patients with COVID-19 have more than 140 inflammatory cytokines activated and this relates to the disease severity, progression, and the hyperactivation of T cells. In viral diseases, an abnormal pro-inflammatory factor release damages the lung physiology and causes oxygen deprivation. This is primed by the unregulated fabrication of a high risk of inflammatory factors like interleukin members, as well as also increasing the level of CRS and chemokines. Cytokines activate the JAK-STAT and Ras-MAPK pathways and stimulate the CRP value, the clear marker used to show infection in the body. On the other hand, for cytokines, an interleukin member is required for lymphocyte growth and development. Treatments which have been shown to effectively reestablish lymphocyte count in a variety of viral infections have been safely delivered to septic shock patients with lymphocyte abnormalities comparable to those seen in COVID-19. Many therapies have been approved and some are under trial for the effective treatment of viral infections including Tocilizumab and Siltuximab.
Introduction
Coronaviruses are enclosed, single-stranded massive RNA viruses with a positive single-stranded RNA strand in living organisms 1 . Coronaviruses are subdivided into four subfamilies; α, β, δ, and Δ. While α and β coronaviruses are assumed to have originated in mammals like bats, the δ and Δ viruses are primarily found in some mammals and aves specie. The genome size ranges from 26 to 32 kb. Among these subfamilies, more than six coronavirus subtypes are able to infect humans. Beta coronaviruses can potentially cause illness and death, while alpha coronaviruses generate asymptomatic or mildly indicative infections. SARS-CoV-2 is a beta coronavirus of the B lineage that is usually correlated to the SARS-CoV virus 1 , 2 .
The key four viral genomes transcribe diverse N, S, SMP, and M, with HKU1 beta coronaviruses exposing a transitory membrane glycoprotein (HE) 3 . Pneumonia was an early diagnostic sign of the SARS-CoV-2-accompanying infection COVID-19, according to Chan JF and his colleagues. GI symptoms and asymptomatic infections have also been reported in modern investigations, especially in younger nurslings 4 . SARS-CoV-2, like many other viruses, infects the alveolar epithelial cells in the lungs through receptor-mediated endocytosis with the ACE2 serving as an entrance receptor 2 .
COVID-19 spreads through a systemic inflammation triggered by immune system hyperactivity in reaction to the virus infection. Lung tissue loss, pulmonary-edema fluid exudation, dyspnea, and pulmonary illness can develop from this persistent inflammation 5 . When compared to healthy lungs, the coronavirus produces a significant decrease in alveolar lacunar space, enhanced immune infiltration, and cell death through apoptosis 6 . COVID-19 decreases the number of lymphocytes in the peripheral blood while elevating the provocative cytokine concentration in the serum. In extreme COVID-19 cases, cytokines, which are most presumably produced by inflammatory monocytes, may be responsible for considerable lung inflammation and pulmonary function deterioration 7 .
In the case of COVID-19, these inflammatory cytokine markers help to diagnose the disease progression and sternness 8 . A cytokine storm is an immunological state marked by prompt propagation and the hyperactivation of T cells (white blood cells), macrophages, natural killer cells (NK cells), and increased production of more than 140 inflammatory markers with biochemical mediators secreted by immune and non-immune cells 9 , 10 . In viral diseases, an abnormal pro-inflammatory factor release damages the lung physiology and the epithelial cell barrier of the alveoli resulting in vascular discharges, edema, and oxygen deprivation which leads to the irregulated fabrication of pro-inflammatory factors known as IL-6, 8, 1, GM-CSF, as well as chemokines 11 . In the current study, the role of interleukin members in COVID-19 has been evaluated.
Figure 1 . Pathogenicity of COVID-19 and role of IL-6.SARS-CoV-2 mainly penetrates the nostrils, eye, and mouth when enters the host cell via an add-on to their receptors which induces an inflammatory effect . ACE2: angiotensin-converting enzyme, LT: leukotriene, ROS: reactive oxygen spices, CRP: c-reactive protein, TNF-α: tumor necrosis factor-alpha, IFN-I: interferon type I, IL-6: interleukin6, IL-6R: interleukin-6 receptor, ARDS: acute respiratory distress syndrome.

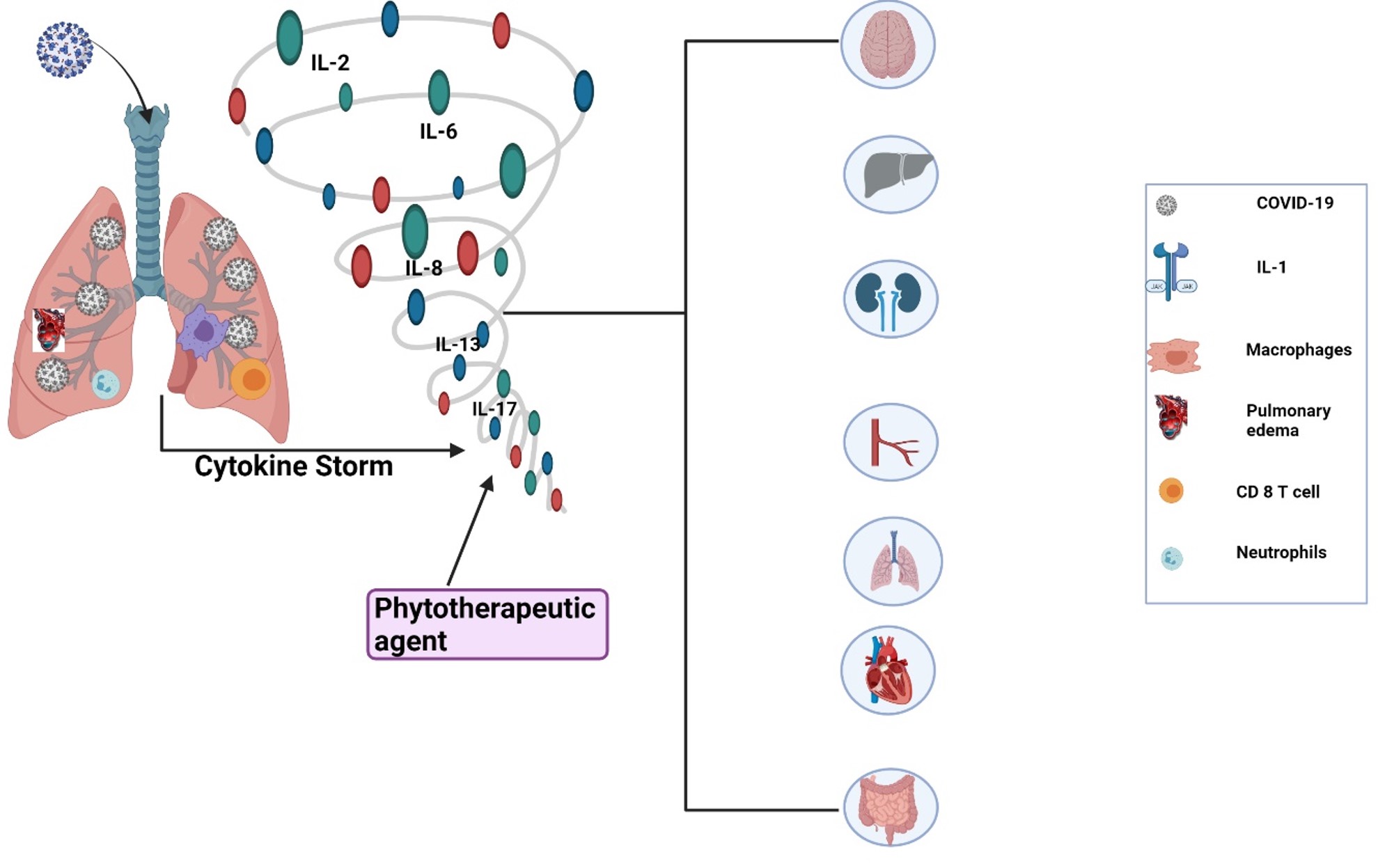
Figure 2 . The spectrum of the destruction of different body organs by cytokine storm (interleukin family) produced during COVID-19.
Role of interleukin-6 (IL-6)
Multiple roles are served by IL-6 and it was initially discovered as a B-cell developmental factor involved in the maturation of immune response cells. Since then, it has been shown that IL-6 has a diverse variety of potential functions, including effects on T cells, blood vessels, and neurons 12 .
During the acute phase of viral infection, there is a systemic amplification of IL-6 and it has pleiotropic protein that is generated and comes back to tissue trauma and microbial infections. Fibroblasts, keratinocytes (skin cells), mesangial cells, vascular endothelial cells, mast cells (also known as mastocytes), macrophages, dendritic cells (nerve cells), and T and B cells (WBCs) are among the cell types that produce cytokine. In COVID-19, this leads to the patient's lungs being destroyed 13 , 14 , 15 .
Several studies have found that IL-6 is significant in the immune-pathogenesis of COVID-19, as indicated by the distinguished blood concentration of this cytokine, particularly in extreme situations 16 , 17 , 18 , 19 . Huang et al . reported higher IL-6 echelons in the case of COVID-19. It interacts through a polypeptide chain called the IL-6 receptor (IL-6R), which subsequently binds to a membrane glycoprotein called gp130 to activate intracellular signaling via the JAK-STAT and Ras-MAPK pathways 18 . In the body, like the central compartment and excretory products such as urine, a soluble derivative of IL-6R (sIL-6 R) is also present. sIL-6 R is generated from a disinterring and metalloprotease17 degradation of IL-6 R 20 . The activation of IL-6 channels promotes the liver cells to generate and secrete an acute and C-reactive protein (CRP) such as serum amyloid A, fibrinogen, and haptoglobin, which is a glycoprotein complex produced in the liver, and 1-antichymotrypsin while diminishing fibronectin, albumin, and transferrin development 21 . COVID-19 is a condition in which IL-6 plays a critical role since it is implicated in the disease etiology and is clinically correlated with prognosis 22 . Particularly, IL-6 has been shown to be a potential biological indicator in a multitude of infections, including pneumonia of various etiologies. It is frequently used in clinical practice and research 21 , 23 , 24 . Chen et al . reported that an enhanced baseline IL-6 was associated with physiological parameters and the finding of serum SARS-CoV-2 RNAemia which appears to be diagnostic for critical illness. After a comparison of severe patients, it was observed that critically ill patients had about 10-fold higher IL-6 levels and all fatal cases had incredibly high IL-6 levels 25 . The increased starting point of a further provocative surrogate marker, including CRP, lactate dehydrogenase (LDH), ferritin, and D-dimer, as well as chest computed tomography (CT) abnormalities, were also determined to be favorably linked with IL-6. Patients healing from COVID-19 had lower IL-6 levels and improved lung physiology but the IL-6 levels elevated where there was an illness re-exacerbation 26 . Pandolfi et al. stated that in the case of COVID-19, the patients admitted to the ICU had higher IL-6 levels than the other admitted people in poor health 27 . In individuals with SARS-COV-2 infection, IL-6 has a potentially harmful function 28 . Additionally, certain cytokines can induce significant pulmonary destruction by aggregating neutrophils and macrophages in the respiratory tract, resulting in the formation of hyaline membranes and drawn-out concealing of the alveolar barriers, as well as tubule-interstitial destruction 29 .
CRS is defined as an abnormal inflammatory reaction with clinical manifestations varying from a flu-like syndrome to an unregulated systemic inflammatory response and multi-organ disturbance, and it is connected with macrophage activation, T lymphocyte modulation, and endothelial cell amplification, as well as increased inflammatory cytokine production. IL-6 is linked to cardiomyopathy, the hastening of complement and coagulation pathways, disseminated intravascular coagulation, and vascular leakage among some of the discharged cytokines. CRS is most common in people who have received various types of immunotherapy or haploidentical allogeneic hematopoietic cell transplantation; nonetheless, COVID-19 patients may develop a CRS-like condition 30 , 31 .
The deadly consequences of COVID-19 may be due to increased cytokine levels. Various putative therapeutics targeting the host immune system, such as inflammatory cytokine inhibition, stem cell therapy, immune cell reduction, postpartum plasma transfusion, and false extracorporeal liver sustenance, may be beneficial in the treatment of COVID-19 32 . The blocking of IL-6 is a potential therapy used for COVID-induced CRS because its level is already reported in COVID-19 cases 33 . As a result, targeting IL-6 for COVID-induced CRS could be beneficial as shown in Table 1 .
Interleukin-7 (IL-7)
Interleukin-7 (IL-7) was discovered more than a decade ago 55 . The human IL-7 gene was detected on chromosome 8q12-13 56 . IL-7 is a cytokine secreted by stromal cells in the lymphoid organs which are essential for T cell growth and survival in the periphery. Exogenous stimulation has little effect on IL-7 secretion by the stromal cells, unlike most other cytokines that act on lymphocytes 57 . This pleiotropic or multiple effected interleukin-7 (IL-7) is required for lymphocytic growth and its survival 58 . Rich and Leder reported that the level of T cells increases as the IL-7 level increases 59 , 60 .
COVID-19 is recognized as a consecutive lymphocyte destroyer since substantial long-term lymphopenia is a close universal observation in individuals with severe COVID-19, and it is linked to increased morbidity and mortality 58 . Putative cytokine interleukin 7 (IL-7) is required for the growth and development of lymphocytic cells 61 , 62 . Interleukin-7 (IL-7) treatments, which have been shown to effectively reestablish lymphocyte count in a variety of viral infections, has been safely delivered in septic shock patients with lymphocyte abnormalities comparable to those seen in COVID-19 63 . Francois et al. saw that IL-7 can be safely administered to critically ill COVID-19 patients without inducing inflammation or pulmonary harm, and it is the marker of immunosuppression that should be severely considered when using IL-7 alone or in combination with other treatments 58 . In addition, the plasma expression levels of IL-2, 7, and 10, granulocyte colony-stimulating factor (GCSF), IP-10, MCP-1, macrophage inflammatory protein-1a (MIP-1A), and tumor necrosis factor (TNF-alpha) are increased in critical care patients with significant illnesses compared to non-ICU patients 43 .
Interleukin-8 (IL-8)
IL-8 concentration was found to be more accurate in the diagnosis of the progression of COVID-19 disease from acute to chronic than IL-7. Both mild and severe COVID-19 patients had elevated IL-8 plasma levels which increased as the disease progressed. IL-8 could therefore be cast as a biomarker for COVID-19 patients in various stages of the disease. Lili et al. reported that the IL-8 levels in the blood were much greater in these people which makes it an excellent indicator of the COVID-19 sickness prognosis 64 . IL-8 is a pro-inflammatory mediator that has been implicated in tissue damage and can drive neutrophils to infected areas 64 . It has been documented in the topical investigation of SARS-CoV-2 infection which could enlighten the lesser manifestation of IL-8. This is crucial for chemo-attraction and neutrophil viability 65 . IL-8 is a proinflammatory cytokine generated by blood cells and a variety of organs, and increased concentrations of IL-8 in the blood have been linked to a variety of disorders 66 . The link between IL-8 and disease duration could point to a function of IL-8 signaling in COVID-19 evolution. According to new research, the onset of polymorphonuclear-myeloid-derived suppressor cells (PMN-MDSC) curtails SARS-CoV-2 specific to the T-cell responses, and the presence of PMN-MDSC at the beginning of treatment is linked to a fatal outcome in COVID-19 patients with a higher intensity of PMN-MDSC in the patients among the non-survivor group compared with the survivor group 67 .
Interleukin 10 (IL-10)
A type II cytokine is interleukin-10 (IL-10). The intron–exon genomic arrangement is analogous to that of other types of cytokines, and they fix to receptors with identical buildings in certain cases. The origin of the IL-10 gene in human chromosome 1q21–32 is made up of more than four axons divided by four introns 68 . T-helper type 2 (Th2) cells are a subgroup of regulatory white blood cell T cells called Tr1, Th1, and Th17 cells. These cells are the four key T-cell carriers of IL-10 69 . Other types of white blood cell such as human B cells and some granulocytes such as eosinophils and mast cells are possible sources of IL-10. Non-immune cell producers of IL-10 are epithelial cells, tumor cells, and keratinocytes 70 , 71 , 72 , 73 .
In severe critically ill patients of COVID-19, the value of interleukin-10 is dramatically increased 74 . The tendency of SARS-CoV-2 infection to trigger IL-10 transcription in SARS-CoV. However, the significance of IL-10 as a potential immunological indicator when assessing the complexity of COVID-19 disease has been discovered 75 , 76 . Long thought to be an anti-inflammatory or immunological inhibitory mechanism generated by a vicious cycle of proinflammatory cytokines, the presence of IL-10 in COVID-19 patients means that the serum has been suspected 76 , 77 . Furthermore, certain researchers have advocated that recombinant IL-10 should be used as an ARDS therapy in COVID-19 patients because of its immunoregulatory and antifibrotic properties 78 .
In COVID-19 patients, there is the involvement of various pro-inflammatory intermediaries and vital organ demolition 79 . The rate of mortality could be reduced by targeting IL-10. COVID-19 individuals with severe/critical illness have drastically high serum IL-10 concentrations which correspond with disease severity 74 . In some critically ill individuals, IL-10 may worsen the viral sepsis-related hyper-inflammation. COVID-19 infected patients 80 .
IL-10 is mostly considered part of the down-regulation of the adaptive T cell response in the beginning 81 , 82 . Xiaoling et al . reported that the inhibition of IL-10 signaling in COVID-19 results in extreme lung inflammation, passiveness, or constructive antiviral immunity 83 .
Interleukin-11
Interleukin-11 is a cytokine released by osteoblasts, fibroblasts, chondrocytes, trophoblasts, and a variety of other signaling pathways in culture 84 . IL-11 is easily noticeable during virally generated inflammation 85 . IL-11 expression can be produced by disease stimuli, implying that it can be induced by pathological stimuli as well 84 .
The more restricted expression pattern of the matching receptor subunits determines IL-11. IL-11R1 is produced in low levels in the central nervous system, respiratory system, thymus, spleen, cardiovascular system, bladder, kidney, muscle, small and large gut, salivary glands, bone marrow, gonads, and uterus among the two transmembrane IL-11R sub-types 84 . IL-11 controls blood disease and bone metabolism and prevents pro-inflammatory cytokine generation 86 . It's worth noting that during the early stages of SRAS-CoV infection, thrombocytopenia and lymphopenia are frequently detected in COVID-19 patients 86 .
Interleukin-13
Giancarlo et al. reported that IL-13 is involved in several activities such as (i) eosinophil, M2 macrophage mobilization to the lungs, (ii) the release of mucus in the air pathway and goblet cell metaplasia, (iii) enhancing the multiplication of smooth muscles, and (iv) the undergoing of fibrosis through fibroblast activation and subsequent collagen deposition 87 . Donlan et al . reported that IL-13 functions as a coordinator of pathogenic mechanisms in the lung. In COVID-19 positive individuals, the plasma altitudes of IL-13 were considerably greater than in uninfected patients 88 .
Patients with acute to chronic asthma have higher amounts of IL-13 in their bronchoalveolar lavage fluid, as well as a higher gene and protein expression in their bronchial mucosal tissues 89 . IL-13 also promotes the release of periostin, a multicellular protein involved in fibroblast stimulation and collagen gel suppleness 90 . To summarize, while IL-13 plays an important part in the pathobiology of asthma, there may be several redundant processes that limit the therapeutic benefits of focusing just on IL-13 91 .
Conclusion
In a viral infection, many cytokine mediators are stimulated to increase secretion and to cause a heightened severity and virulence in the body which leads to causing CRS and a high value of CRP. Many therapies are effective against CRS and harm cytokines which help to minimize the viral infection in the body. However, due to the notorious activity and physiology of virus activity, there is a need to engage in more trials and to study effective therapies.
Abbreviations
ARDS : Acute respiratory distress syndrome
CRP : C-reactive protein
CRS : Cytokine release syndrome
GCSF : Granulocyte colony-stimulating factor
PMN-MDSC : polymorphonuclear- 218 myeloid-derived suppressor cells
TNF-alpha : Tumor necrosis factor-alpha
Acknowledgments
The authors thank full to the Vice-Chancellor University of Okara. All figures were originally drawn on Biorender.com.
Author’s contributions
All authors significantly contributed to this work, read and approved the final manuscript.
Funding
None.
Availability of data and materials
Not applicable.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
References
- Velavan T.P., Meyer C.G.. The COVID-19 epidemic. Tropical Medicine & International Health. 2020;25(3):278-80. View Article PubMed Google Scholar
- Zhou P., Yang X.-L., Wang X.-G., Hu B., Zhang L., Zhang W.. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579(7798):270-273. Google Scholar
- Rottier P.J.. The coronavirus membrane glycoprotein. InThe coronaviridae 1995 (pp. 115-139). Springer, Boston, MA.. .
- Chan J.F., Yuan S., Kok K.H., To K.K., Chu H., Yang J.. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 2020;395(10223):514-23. View Article PubMed Google Scholar
- Rendeiro A.F., Ravichandran H., Bram Y., Chandar V., Kim J., Meydan C.. The spatial landscape of lung pathology during COVID-19 progression. Nature. 2021;593(7860):564-9. View Article PubMed Google Scholar
- Grasselli G., Tonetti T., Protti A., Langer T., Girardis M., Bellani G., collaborators Pathophysiology of COVID-19-associated acute respiratory distress syndrome: a multicentre prospective observational study. The Lancet. Respiratory Medicine. 2020;8(12):1201-8. View Article PubMed Google Scholar
- Liu B., Li M., Zhou Z., Guan X., Xiang Y.. Can we use interleukin-6 (IL-6) blockade for coronavirus disease 2019 (COVID-19)-induced cytokine release syndrome (CRS)?. Journal of Autoimmunity. 2020;111:102452. View Article PubMed Google Scholar
- Del Valle D.M., Kim-Schulze S., Huang H.H., Beckmann N.D., Nirenberg S., Wang B.. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nature Medicine. 2020;26(10):1636-43. View Article PubMed Google Scholar
- Osterholm M.T.. Preparing for the next pandemic. The New England Journal of Medicine. 2005;352(18):1839-42. View Article PubMed Google Scholar
- Teijaro J.R., Walsh K.B., Rice S., Rosen H., Oldstone M.B.. Mapping the innate signaling cascade essential for cytokine storm during influenza virus infection. Proceedings of the National Academy of Sciences of the United States of America. 2014;111(10):3799-804. View Article PubMed Google Scholar
- Reghunathan R., Jayapal M., Hsu L.Y., Chng H.H., Tai D., Leung B.P.. Expression profile of immune response genes in patients with Severe Acute Respiratory Syndrome. BMC Immunology. 2005;6(1):2. View Article PubMed Google Scholar
- Cronstein B.N.. Interleukin-6. Bulletin of the NYU Hospital for Joint Diseases. 2007;65(1):11-5. PubMed Google Scholar
- Mauer J., Denson J.L., Brüning J.C.. Versatile functions for IL-6 in metabolism and cancer. Trends in Immunology. 2015;36(2):92-101. View Article PubMed Google Scholar
- Tanaka T., Narazaki M., Kishimoto T.. IL-6 in inflammation, immunity, and disease. Cold Spring Harbor Perspectives in Biology. 2014;6(10):a016295. View Article PubMed Google Scholar
- Smetana K., Brábek J.. Role of interleukin-6 in lung complications in patients with COVID-19: Therapeutic implications. In vivo. 2020;34(3 suppl):1589-1592. Google Scholar
- Liu Y., Zhang C., Huang F., Yang Y., Wang F., Yuan J.. Elevated plasma levels of selective cytokines in COVID-19 patients reflect viral load and lung injury. National Science Review. 2020;7(6):1003-11. View Article PubMed Google Scholar
- Liu J., Li S., Liu J., Liang B., Wang X., Wang H.. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine. 2020;55:102763. View Article PubMed Google Scholar
- Huang Y., Tu M., Wang S., Chen S., Zhou W., Chen D.. Clinical characteristics of laboratory confirmed positive cases of SARS-CoV-2 infection in Wuhan, China: A retrospective single center analysis. Travel Medicine and Infectious Disease. 2020;36:101606. View Article PubMed Google Scholar
- Ruan Q., Yang K., Wang W., Jiang L., Song J.. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Medicine. 2020;46(5):846-8. View Article PubMed Google Scholar
- Müllberg J., Schooltink H., Stoyan T., Günther M., Graeve L., Buse G.. The soluble interleukin-6 receptor is generated by shedding. European Journal of Immunology. 1993;23(2):473-80. View Article PubMed Google Scholar
- Unver N., McAllister F.. IL-6 family cytokines: key inflammatory mediators as biomarkers and potential therapeutic targets. Cytokine {&}amp; Growth Factor Reviews. 2018;41:10-7. View Article PubMed Google Scholar
- Potere N., Batticciotto A., Vecchié A., Porreca E., Cappelli A., Abbate A.. The role of IL-6 and IL-6 blockade in COVID-19. Expert Review of Clinical Immunology. 2021;17(6):601-18. View Article PubMed Google Scholar
- Ryabkova V.A., Churilov L.P., Shoenfeld Y.. Influenza infection, SARS, MERS and COVID-19: cytokine storm - The common denominator and the lessons to be learned. Clinical Immunology (Orlando, Fla.). 2021;223:108652. View Article PubMed Google Scholar
- Jones S.A., Jenkins B.J.. Recent insights into targeting the IL-6 cytokine family in inflammatory diseases and cancer. Nature Reviews. Immunology. 2018;18(12):773-89. View Article PubMed Google Scholar
- Chen X., Zhao B., Qu Y., Chen Y., Xiong J., Feng Y.. Detectable serum severe acute respiratory syndrome coronavirus 2 viral load (RNAemia) is closely correlated with drastically elevated interleukin 6 level in critically ill patients with coronavirus disease 2019. Clinical Infectious Diseases. 2020;71(8):1937-42. View Article PubMed Google Scholar
- Liu T., Zhang J., Yang Y., Ma H., Li Z., Zhang J.. The role of interleukin-6 in monitoring severe case of coronavirus disease 2019. EMBO Molecular Medicine. 2020;12(7):e12421. View Article PubMed Google Scholar
- Pandolfi L., Fossali T., Frangipane V., Bozzini S., Morosini M., D'Amato M.. Broncho-alveolar inflammation in COVID-19 patients: a correlation with clinical outcome. BMC Pulmonary Medicine. 2020;20(1):301. View Article PubMed Google Scholar
- Chen W., Lan Y., Yuan X., Deng X., Li Y., Cai X.. Detectable 2019-nCoV viral RNA in blood is a strong indicator for the further clinical severity. Emerging Microbes & Infections. 2020;9(1):469-73. View Article PubMed Google Scholar
- Magro G.. SARS-CoV-2 and COVID-19: is interleukin-6 (IL-6) the `culprit lesion' of ARDS onset? What is there besides Tocilizumab? SGP130Fc. Cytokine: X. 2020;2(2):100029. View Article PubMed Google Scholar
- Bhaskar S., Sinha A., Banach M., Mittoo S., Weissert R., Kass J.S.. Cytokine storm in COVID-19 immunopathological mechanisms, clinical considerations, and therapeutic approaches: the REPROGRAM consortium position paper. Frontiers in Immunology. 2020;11:1648. View Article PubMed Google Scholar
- A Shimabukuro-Vornhagen, P Gödel, M Subklewe, HJ Stemmler, HA Schlößer, M Schlaak. Cytokine release syndrome. Journal for immunotherapy of cancer. 2018;6(1):1-14. Google Scholar
- Chen C., Zhang X., Ju Z., He W.. Advances in the research of cytokine storm mechanism induced by Corona Virus Disease 2019 and the corresponding immunotherapies. Zhonghua shao shang za zhi= Zhonghua shaoshang zazhi= Chinese journal of burns. 2020;36:E005-E. Google Scholar
- Liu B., Li M., Zhou Z., Guan X., Xiang Y.. Can we use interleukin-6 (IL-6) blockade for coronavirus disease 2019 (COVID-19)-induced cytokine release syndrome (CRS)?. Journal of Autoimmunity. 2020;111:102452. View Article PubMed Google Scholar
- Choy E.H., Isenberg D.A., Garrood T., Farrow S., Ioannou Y., Bird H.. Therapeutic benefit of blocking interleukin-6 activity with an anti-interleukin-6 receptor monoclonal antibody in rheumatoid arthritis: a randomized, double-blind, placebo-controlled, dose-escalation trial. Arthritis and Rheumatism. 2002;46(12):3143-50. View Article PubMed Google Scholar
- Sukumaran S., Watanabe N., Bajgain P., Raja K., Mohammed S., Fisher W.E.. Enhancing the potency and specificity of engineered T cells for cancer treatment. Cancer Discovery. 2018;8(8):972-87. View Article PubMed Google Scholar
- Nakaoka Y., Isobe M., Takei S., Tanaka Y., Ishii T., Yokota S.. Efficacy and safety of tocilizumab in patients with refractory Takayasu arteritis: results from a randomised, double-blind, placebo-controlled, phase 3 trial in Japan (the TAKT study). Annals of the Rheumatic Diseases. 2018;77(3):348-54. View Article PubMed Google Scholar
- Villiger P.M., Adler S., Kuchen S., Wermelinger F., Dan D., Fiege V.. Tocilizumab for induction and maintenance of remission in giant cell arteritis: a phase 2, randomised, double-blind, placebo-controlled trial. Lancet. 2016;387(10031):1921-7. View Article PubMed Google Scholar
- Aletaha D., Bingham C.O., Tanaka Y., Agarwal P., Kurrasch R., Tak P.P.. Efficacy and safety of sirukumab in patients with active rheumatoid arthritis refractory to anti-TNF therapy (SIRROUND-T): a randomised, double-blind, placebo-controlled, parallel-group, multinational, phase 3 study. Lancet. 2017;389(10075):1206-17. View Article PubMed Google Scholar
- Mease P.J., Gottlieb A.B., Berman A., Drescher E., Xing J., Wong R.. The efficacy and safety of clazakizumab, an anti\textendashinterleukin-6 monoclonal antibody, in a phase IIb study of adults with active psoriatic arthritis. Arthritis & Rheumatology (Hoboken, N.J.). 2016;68(9):2163-73. View Article PubMed Google Scholar
- Khanna D., Denton C.P., Jahreis A., van Laar J.M., Frech T.M., Anderson M.E.. Safety and efficacy of subcutaneous tocilizumab in adults with systemic sclerosis (faSScinate): a phase 2, randomised, controlled trial. Lancet. 2016;387(10038):2630-40. View Article PubMed Google Scholar
- Raimondo M.G., Biggioggero M., Crotti C., Becciolini A., Favalli E.G.. Profile of sarilumab and its potential in the treatment of rheumatoid arthritis. Drug Design, Development and Therapy. 2017;11:1593-603. View Article PubMed Google Scholar
- Bennett T.D., Fluchel M., Hersh A.O., Hayward K.N., Hersh A.L., Brogan T.V.. Macrophage activation syndrome in children with systemic lupus erythematosus and children with juvenile idiopathic arthritis. Arthritis and Rheumatism. 2012;64(12):4135-42. View Article PubMed Google Scholar
- Henter J.I., Horne A., Aricó M., Egeler R.M., Filipovich A.H., Imashuku S.. HLH-2004: diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatric Blood & Cancer. 2007;48(2):124-31. View Article PubMed Google Scholar
- de Wilde A.H., Zevenhoven-Dobbe J.C., van der Meer Y., Thiel V., Narayanan K., Makino S.. Cyclosporin A inhibits the replication of diverse coronaviruses. The Journal of General Virology. 2011;92(Pt 11):2542-8. View Article PubMed Google Scholar
- Rochwerg B., Oczkowski S.J., Siemieniuk R.A., Agoritsas T., Belley-Cote E., D'Aragon F.. Corticosteroids in sepsis: an updated systematic review and meta-analysis. Critical Care Medicine. 2018;46(9):1411-20. View Article PubMed Google Scholar
- Hamid U., Krasnodembskaya A., Fitzgerald M., Shyamsundar M., Kissenpfennig A., Scott C.. Aspirin reduces lipopolysaccharide-induced pulmonary inflammation in human models of ARDS. Thorax. 2017;72(11):971-80. View Article PubMed Google Scholar
- Ocon A.J., Bhatt B.D., Miller C., Peredo R.A.. Safe usage of anakinra and dexamethasone to treat refractory hemophagocytic lymphohistiocytosis secondary to acute disseminated histoplasmosis in a patient with HIV/AIDS. Case Reports. 2017;2017:bcr-2017-221264. Google Scholar
- Rojas N.C.. Efficacité et tolérance des agents biologiques dans les rhumatismes inflammatoires à début juvénile dans les essais cliniques randomisés et les études observationnelles: Université de Lyon; 2019.. . ;:. Google Scholar
- Canna S.W., Girard C., Malle L., de Jesus A., Romberg N., Kelsen J.. Life-threatening NLRC4-associated hyperinflammation successfully treated with IL-18 inhibition. The Journal of Allergy and Clinical Immunology. 2017;139(5):1698-701. View Article PubMed Google Scholar
- van Rhee F., Wong R.S., Munshi N., Rossi J.F., Ke X.Y., Foss\aa A.. Siltuximab for multicentric Castleman's disease: a randomised, double-blind, placebo-controlled trial. The Lancet. Oncology. 2014;15(9):966-74. View Article PubMed Google Scholar
- De Benedetti F., Brunner H., Ruperto N., Schneider R., Xavier R., Allen R., Paediatric Rheumatology International Trials Organisation the Pediatric Rheumatology Collaborative Study Group Catch-up growth during tocilizumab therapy for systemic juvenile idiopathic arthritis: results from a phase III trial. Arthritis {&}amp; Rheumatology (Hoboken, N.J.). 2015;67(3):840-8. View Article PubMed Google Scholar
- Nishimoto N., Kanakura Y., Aozasa K., Johkoh T., Nakamura M., Nakano S.. Humanized anti-interleukin-6 receptor antibody treatment of multicentric Castleman disease. Blood. 2005;106(8):2627-32. View Article PubMed Google Scholar
- Jones G., Sebba A., Gu J., Lowenstein M.B., Calvo A., Gomez-Reino J.J.. Comparison of tocilizumab monotherapy versus methotrexate monotherapy in patients with moderate to severe rheumatoid arthritis: the AMBITION study. Annals of the Rheumatic Diseases. 2010;69(1):88-96. View Article PubMed Google Scholar
- Kaneko Y., Kameda H., Ikeda K., Ishii T., Murakami K., Takamatsu H.. Tocilizumab in patients with adult-onset still's disease refractory to glucocorticoid treatment: a randomised, double-blind, placebo-controlled phase III trial. Annals of the Rheumatic Diseases. 2018;77(12):1720-9. View Article PubMed Google Scholar
- Fry T.J., Mackall C.L.. Interleukin-7: from bench to clinic. Blood. 2002;99(11):3892-904. View Article PubMed Google Scholar
- Sutherland G.R., Baker E., Fernandez K.E., Callen D.F., Goodwin R.G., Lupton S.. The gene for human interleukin 7 (IL7) is at 8q12-13. Human Genetics. 1989;82(4):371-2. View Article PubMed Google Scholar
- Mazzucchelli R., Durum S.K.. Interleukin-7 receptor expression: intelligent design. Nature Reviews. Immunology. 2007;7(2):144-54. View Article PubMed Google Scholar
- Laterre P.F., François B., Collienne C., Hantson P., Jeannet R., Remy K.E.. Association of interleukin 7 immunotherapy with lymphocyte counts among patients with severe coronavirus disease 2019 (COVID-19). JAMA network open. 2020;3(7):e2016485-e. Google Scholar
- Geiselhart L.A., Humphries C.A., Gregorio T.A., Mou S., Subleski J., Komschlies K.L.. IL-7 administration alters the CD4:CD8 ratio, increases T cell numbers, and increases T cell function in the absence of activation. Journal of Immunology (Baltimore, Md.: 1950). 2001;166(5):3019-27. View Article PubMed Google Scholar
- Rich B.E., Leder P.. Transgenic expression of interleukin 7 restores T cell populations in nude mice. The Journal of Experimental Medicine. 1995;181(3):1223-8. View Article PubMed Google Scholar
- Barata J.T., Durum S.K., Seddon B.. Flip the coin: IL-7 and IL-7R in health and disease. Nature Immunology. 2019;20(12):1584-93. View Article PubMed Google Scholar
- Mackall C.L., Fry T.J., Gress R.E.. Harnessing the biology of IL-7 for therapeutic application. Nature Reviews. Immunology. 2011;11(5):330-42. View Article PubMed Google Scholar
- Monneret G., Cour M., Viel S., Venet F., Argaud L.. Coronavirus disease 2019 as a particular sepsis: a 2-week follow-up of standard immunological parameters in critically ill patients. Intensive Care Medicine. 2020;46(9):1764-5. View Article PubMed Google Scholar
- Li L., Li J., Gao M., Fan H., Wang Y., Xu X.. Interleukin-8 as a biomarker for disease prognosis of coronavirus disease-2019 patients. Frontiers in Immunology. 2020;\textbullet\textbullet\textbullet:11. PubMed Google Scholar
- Azevedo M.L., Zanchettin A.C., Vaz de Paula C.B., Motta Júnior J.D., Malaquias M.A., Raboni S.M.. Lung Neutrophilic Recruitment and IL-8/IL-17A Tissue Expression in COVID-19. Frontiers in Immunology. 2021;12:656350. View Article PubMed Google Scholar
- Shahzad A., Knapp M., Lang I., Köhler G.. Interleukin 8 (IL-8) - a universal biomarker?. International Archives of Medicine. 2010;3(1):11. View Article PubMed Google Scholar
- Sacchi A., Grassi G., Bordoni V., Lorenzini P., Cimini E., Casetti R.. Early expansion of myeloid-derived suppressor cells inhibits SARS-CoV-2 specific T-cell response and may predict fatal COVID-19 outcome. Cell Death {&}amp; Disease. 2020;11(10):921. View Article PubMed Google Scholar
- Mosser D.M., Zhang X.. Interleukin-10: new perspectives on an old cytokine. Immunological Reviews. 2008;226(1):205-18. View Article PubMed Google Scholar
- O'Garra A., Vieira P.. T(H)1 cells control themselves by producing interleukin-10. Nature Reviews. Immunology. 2007;7(6):425-8. View Article PubMed Google Scholar
- Fillatreau S., Gray D., Anderton S.M.. Not always the bad guys: B cells as regulators of autoimmune pathology. Nature Reviews. Immunology. 2008;8(5):391-7. View Article PubMed Google Scholar
- JJ Ryan, M Kashyap, D Bailey, S Kennedy, K Speiran, J Brenzovich. Mast cell homeostasis: a fundamental aspect of allergic disease. Critical Reviews in Immunology. 2007;27(1):. View Article Google Scholar
- Moore K.W., de Waal Malefyt R., Coffman R.L., O'Garra A.. Interleukin-10 and the interleukin-10 receptor. Annual Review of Immunology. 2001;19(1):683-765. View Article PubMed Google Scholar
- Williams L.M., Ricchetti G., Sarma U., Smallie T., Foxwell B.M.. Interleukin-10 suppression of myeloid cell activation - a continuing puzzle. Immunology. 2004;113(3):281-92. View Article PubMed Google Scholar
- Lu L., Zhang H., Dauphars D.J., He Y.W.. A Potential Role of Interleukin-10 in COVID-19 Pathogenesis. Trends in Immunology. 2020;42(1):3-5. PubMed Google Scholar
- Han H., Ma Q., Li C., Liu R., Zhao L., Wang W.. Profiling serum cytokines in COVID-19 patients reveals IL-6 and IL-10 are disease severity predictors. Emerging Microbes {&}amp; Infections. 2020;9(1):1123-30. View Article PubMed Google Scholar
- Zhao Y., Qin L., Zhang P., Li K., Liang L., Sun J.. Longitudinal COVID-19 profiling associates IL-1RA and IL-10 with disease severity and RANTES with mild disease. JCI Insight. 2020;5(13):139834. View Article PubMed Google Scholar
- Diao B., Wang C., Tan Y., Chen X., Liu Y., Ning L.. Reduction and functional exhaustion of T cells in patients with coronavirus disease 2019 (COVID-19). Frontiers in Immunology. 2020;11:827. View Article PubMed Google Scholar
- Hu W.-C.. Use interleukin-10 as the therapeutic agent for COVID-19. . 2020;:. View Article Google Scholar
- Lu L., Zhang H., Zhan M., Jiang J., Yin H., Dauphars D.J.. Preventing mortality in COVID-19 patients: which cytokine to target in a raging storm?. Frontiers in Cell and Developmental Biology. 2020;8:677. View Article PubMed Google Scholar
- Li H., Liu L., Zhang D., Xu J., Dai H., Tang N.. SARS-CoV-2 and viral sepsis: observations and hypotheses. Lancet. 2020;395(10235):1517-20. View Article PubMed Google Scholar
- Saraiva M., Vieira P., O'Garra A.. Biology and therapeutic potential of interleukin-10. The Journal of Experimental Medicine. 2020;217(1):e20190418. View Article PubMed Google Scholar
- Ouyang W., O'Garra A.. IL-10 family cytokines IL-10 and IL-22: from basic science to clinical translation. Immunity. 2019;50(4):871-91. View Article PubMed Google Scholar
- Xu X., Han M., Li T., Sun W., Wang D., Fu B.. Effective treatment of severe COVID-19 patients with tocilizumab. Proceedings of the National Academy of Sciences of the United States of America. 2020;117(20):10970-5. View Article PubMed Google Scholar
- Putoczki T., Ernst M.. More than a sidekick: the IL-6 family cytokine IL-11 links inflammation to cancer. Journal of Leukocyte Biology. 2010;88(6):1109-17. View Article PubMed Google Scholar
- Zheng T., Zhu Z., Wang J., Homer R.J., Elias J.A.. IL-11: insights in asthma from overexpression transgenic modeling. The Journal of Allergy and Clinical Immunology. 2001;108(4):489-96. View Article PubMed Google Scholar
- Cheng M., Chan C.W., Cheung R.C., Bikkavilli R.K., Zhao Q., Au S.W.. Cross-reactivity of antibody against SARS-coronavirus nucleocapsid protein with IL-11. Biochemical and Biophysical Research Communications. 2005;338(3):1654-60. View Article PubMed Google Scholar
- Marone G., Granata F., Pucino V., Pecoraro A., Heffler E., Loffredo S.. The intriguing role of interleukin 13 in the pathophysiology of asthma. Frontiers in Pharmacology. 2019;10:1387. View Article PubMed Google Scholar
- Donlan A.N., Young M., Petri W.A., Abhyankar M.. IL-13 predicts the need for mechanical ventilation in COVID-19 patients. medRxiv. medRxiv. 2020;:. View Article Google Scholar
- Saha S.K., Berry M.A., Parker D., Siddiqui S., Morgan A., May R.. Increased sputum and bronchial biopsy IL-13 expression in severe asthma. The Journal of Allergy and Clinical Immunology. 2008;121(3):685-91. View Article PubMed Google Scholar
- Takayama G., Arima K., Kanaji T., Toda S., Tanaka H., Shoji S.. Periostin: a novel component of subepithelial fibrosis of bronchial asthma downstream of IL-4 and IL-13 signals. The Journal of Allergy and Clinical Immunology. 2006;118(1):98-104. View Article PubMed Google Scholar
- Nair P., O'Byrne P.M.. The interleukin-13 paradox in asthma: effective biology, ineffective biologicals. Eur Respir J. 2019;53(2):1802250. View Article PubMed Google Scholar
- Qin C., Ziwei M.P.L.Z.M., Tao S.Y.M.Y., Ke P.C.X.M.P., Shang M.M.P.K.. Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clin Infect Dis. 2020;71(15):762-768. View Article PubMed Google Scholar
- Mehta P., McAuley D.F., Brown M., Sanchez E., Tattersall R.S., Manson J.J., HLH Across Speciality Collaboration UK. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. 2020;395(10229):1033-4. View Article PubMed Google Scholar