Open Access
Open Access Abstract
Introduction: The most important cause of mortality in the world is cardiovascular disease (CVD). Dysfunction of the endothelium is the initiating and exacerbating cause of atherosclerosis. Acute myocardial infarction (AMI) in patients with a history of diabetes mellitus (DM) leads to a higher mortality and severe disease course.
Methods: The research design included 120 patients: Group 1 – AMI patients and concomitant DM type (n = 70) and Group 2 – AMI patients (n = 50) without concomitant DM type 2. 20 practically healthy persons were part of the reference groups. All patients were treated using instrumental and laboratory examinations in compliance with the current orders of the Ministry of Health of Ukraine.
Results: The average level of ADMA on the first day of the AMI in patients of Group 1 was 1.57 ± 0.11 mmol/l; Group 2 – 0.61 ± 0.06 mmol/l; reference group – 0.17 ± 0.023 mmol/l (p1;2 < 0.00001, p1;3 < 0.001, p2;3 < 0.01). The average level of troponin I on the first day of the AMI in Group 1 was 4.89 ± 2.46 ng/ml; Group 2 – 2.67 ± 2.06 ng/ml; reference group – 0.06 ± 0.04 ng/ml (p1-2 < 0.00001, p1-3 < 0.00001, p2-3 < 0.00001). The direct marked correlation between ADMA and troponin I levels was revealed in the course of the correlation analysis (r = 0.687; p < 0.05).
Conclusion: Asymmetric dimethylarginine is concluded to act as a marker of endothelial dysfunction. This has a high diagnostic value in cases of the acute myocardial infarction, especially where the patients have diabetes mellitus type 2. The research revealed the hyperactivity of troponin I in patients with the examined comorbid pathology. In the course of the correlation analysis, a direct marked correlation was revealed between the levels of asymmetric dimethylarginine and troponin I (p < 0.05). Correlation analysis between the marker of endothelial dysfunction and the marker of myocardial damage in the patients in Group 1 as per the form of diabetes mellitus type 2 demonstrated a direct marked correlation in the case of a mild form of carbohydrate metabolism disorder and a strong correlation in the case of moderate and severe forms of carbohydrate metabolism disorder.
Introduction
Cardiovascular disease (CVD) is the highest cause of mortality worldwide. For the development of an effective and timely strategy to overcome the CVD epidemic, it is necessary to clearly understand the modern epidemiological features of the main types of this disease and the consequences regarding the prevention and treatment of the pathology. Some of the features are related to changes in demographic, environment, lifestyle, and healthcare, including an increase in the percentage of atherosclerotic CVD (coronary heart disease (CHD)), reduced mortality due to hemorrhage, various regional epidemiological trends for the subtypes of these diseases, an increase in the number of patients with stable types of CHD, and age changes in this group of patients. Other features highlight the issues that require special attention, in particular, a high rate of outpatient mortality for the patients with CHD in the case of insufficient prehospital treatment. There are large gaps between the recommended guidelines and goals according to levels of indicator for lifestyle, as well as a large number of patients with untreated, uncontrolled, and undiagnosed hypertension hypercholesterolemia and diabetes mellitus (DM) 1 .
Atherosclerosis is the pathological basis of many types of cardiovascular disease: coronary heart disease, acute myocardial infarction (AMI), and stroke among them. The dysfunction of the endothelium is an initiating and aggravating factor of atherosclerosis. Recent studies link oxidative stress and mitochondrial damage to endothelial dysfunction 2 , 3 , 4 , 5 , 6 .
AMI in patients with DM leads to a higher mortality and more severe course. AMI is a global public health problem that causes irreversible damage to the heart tissue and sudden death, requiring new prevention and treatment strategies 7 .
Hyperglycemia and hypoglycemia are known to be risk factors for CVD development. An examination of 392 DM patients with acute heart failure (AHF) treated in intensive care revealed major cardiovascular events (MACE) in 227 patients (57.9%) including AMI, ischemic stroke, and heart death. In total, 92 patients died from cardiac causes (23.5%) and 107 were hospitalized for heart failure (27.3%), 19 had the first onset of AMI (4.8%), and 9 had an ischemic stroke (2.3%). Logistic multivariate regression analysis showed that glucose level disturbances were associated with the patients older than 75 years old, a reduced indicator of the ejection fraction of the left ventricle (< 30%), and the female gender as the significant predictors of MACE. These were hazard ratio (HR) 3.16 (confidence interval (CI)) 2.25 – 4.43; p < 0.001), HR 1.54 (CI 1.14 – 2.08; p = 0.005), HR 1.47 (CI 1.06 – 2.07; p = 0.02), and HR 1.43 (CI 1.05 – 1.94; p = 0.03), respectively. In this research, it was found that among the other well-known risk factors for the occurrence of heart failure, the importance of glucose level disturbances, especially hyperglycemia, was the strongest independent predictor for medium-term MACE in patients with DM and AHF 8 .
Impaired glycemic level is especially important in acute coronary syndrome (ACS). Gerbaud E. et al . examined patients with DM and ACS (n=327). MACE was observed in 89 patients (27.2%) during the 16.9 months of follow-up. During the follow-up period, 24 patients (7.3%) died of cardiac causes, 35 (10.7%) underwent AMI for the first time, and 30 (9.2%) were hospitalized for ACS. The multifactor logistic regression analysis showed that hyperglycemia and the decreased ejection fraction of the left ventricle (< 40%) were independent predictors of MACE with an odd ratios (ORs) of 2.21 (95% СІ 1.64 – 2.98; p < 0.001) and 1.71 (CI 1.14 – 2.54; p = 0.009), respectively. Thus, hyperglycemia was determined to be the most important independent prognostic factor of medium-term MACE in patients with MD and ACS 9 , 10 , 11 , 12 , 13 , 14 .
Today, bone marrow progenitor endothelial cells are considered to be triggers that promote cardiac neovascularization while exacerbating ischemic injury 15 , 16 , 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 .
The role of the biomarkers of fibrosis and the remodeling of the myocardium (galectin-3, a soluble isoform for the suppression of tumorigenicity 2, matrix metalloproteinases, osteopontin, interleukin-6, syndecan-4, myostatin, procollagen type I C-terminal propeptide, procollagen type III N-terminal propeptide, vascular endothelial growth factor, nitric oxidase synthetase and asymmetric dimethylarginine (ADMA)), myocyte damage (heart-type fatty acid-binding protein, glutathione S-transferase P1, and heat shock protein 60), as the cardiovascular biomarkers of clinical significance and prospectives, are now being studied 28 .
ADMA is an endogenous inhibitor of nitric oxide synthase 29 , 30 , 31 , 32 , a marker related to endothelial dysfunction and atherosclerosis, as well as the illness severity of patients with chronic flammable illnesses 33 .
ADMA is a metabolite of arginine, the determination of which is useful to evaluate cardiovascular disease, kidney disease, and nonalcoholic fatty liver disease 34 .
The increased concentration of ADMA in the blood plasma is connected to the increased risk of mortality and unacceptable cerebrovascular diseases, as is especially evident in the case of AMI 35 , 36 , 37 , 38 , 39 , 40 .
In AMI, the necrotic death of cardiomyocytes occurs, characterized by the rupturing of the sarcolemma in response to a critical level of energy depletion after more than 15 minutes of ischemia. The gold standard, a biomarker for the rapid identification of acute coronary syndrome (ACS), is troponin. Troponin I and troponin T are highly specific and reference the death of cardiomyocytes. It has been proven that in normal ventricular remodeling and pathophysiological conditions, the level of troponin is directly proportional to the degree of myocyte apoptosis 41 .
Methods
In the course of this study, 120 patients were examined who were divided into two groups, specifically one group consisting of AMI patients with concomitant DM type 2 (n = 70) and the second group consisting of AMI patients (n = 50) without concomitant DM type 2. The gender composition of the examined patients consisted of 60 men (50%) and 60 women (50%). The average age of the examined patients was 66.35 ± 0.91 years (p < 0.05). Additionally, 20 practically healthy people were included in the reference group.
Group 1 was divided into 3 subgroups according to the degree of DM type 2: subgroup 1 — a mild form of DM type 2 (5 patients), subgroup 2 — a moderate form of DM type 2 (30 patients), and subgroup 3 — a severe form of DM type 2 (35 patients).
The patients who participated in this research were examined on the basis of the skills of the Municipal Non-Profit Enterprise "City Clinical Hospital No. 27" of Kharkiv City Council (Cardiology Department for patients with acute myocardial infarction) and Kharkiv Railways Clinical Hospital No. 1 of the branch "Health Center" owned by the Joint-Stock Company "Ukrainian Railways" (1 st Cardiology Department).
According to the current orders of the Ministry of Health of Ukraine, the diagnoses of AMI and Type 2 diabetes were established.
According to the orders of the Ministry of Health of Ukraine No. 455 dated 02.07.2014 "Unified clinical protocol of emergency, primary, secondary (specialized) and tertiary (highly specialized) medical care and medical rehabilitation - acute coronary syndrome with an elevation of ST segment" and No. 1957 dated 15.09.2021 "Unified clinical protocol of emergency, primary, secondary (specialized) and tertiary (highly specialized) medical care and medical cardiorehabilitation — Acute coronary syndrome without ST an elevation," a diagnosis of AMI was established.
The diagnosis of DM type 2 was established in compliance with the order of the Ministry of Health No. 1118 dated 21.12.2012 "Unified clinical protocol of primary and secondary (specialized) medical care for patients with diabetes mellitus type 2."
In accordance with the current orders of the Ministry of Health of Ukraine, the sampled patients underwent laboratory and instrumental examinations. The laboratory examinations included the determination of the levels of troponin I, alanine aminotransferase, aspartate aminotransferase, potassium, sodium, bilirubin, creatinine, blood lipid profile (total cholesterol, low-density lipoprotein cholesterol, extra-low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, atherogenic factor, the determination of the marker of endothelial dysfunction — ADMA), blood glucose, general blood, and urine tests twice. The first was on the first day of hospitalization and then 6 months after the coronary event.
This study was conducted in strict compliance with the main ethical provisions of the "Rules of ethical principles of scientific medical research with human participation", approved by the Helsinki Declaration (1964 - 2013), ICH GCP (1996), EEC Directive No. 609 (dated 24.11.1986), orders of the Ministry of Health of Ukraine No. 690 dated 23.09.2009, No. 944 dated 14.12.2009, No. 616 dated 03.08.2012. a). Each patient who participated in this research signed the form of primary accounting documentation No. 003-6/o "Informed voluntary consent of the patient to diagnosis, treatment and surgery, conducting analgesia and presence or participation of the educational process members." Complete anonymity was ensured for each patient.
The statistical processing of the results obtained during the study was carried out using the StatSoft Inc USA software package, "Statistica 6.0." During the research, a standard program of correlation analysis through calculation was used, specifically involving M ± m, probability, and the level of reliability (p) for the comparison of the samples. The analysis of the independent samples not subject to Gaussian distribution laws was performed using the Mann-Whitney U-test. The correlation rate (r) was used to estimate the degree of relationships between the samples.

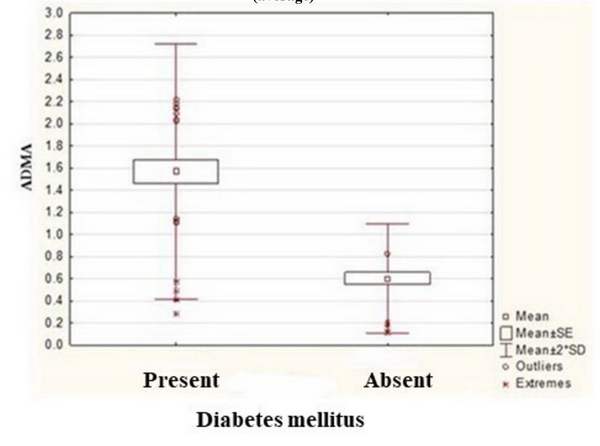
Figure 3 . The average level of ADMA according to the forms diabetes mellitus type 2.

Results
The average level of ADMA in the patients of Group 1 on the first day of AMI was 1.57 ± 0.11 μmol/l, while for Group 2 it was 0.61 ± 0.06 μmol/l and for the reference group, 0.17 ± 0.023 μmol/l (р 1,2 ˂ 0.00001, р 1,3 ˂ 0.001, p 2,3 < 0.01), as shown in Figure 1 , Figure 2 and Table 1 .
For Group 1, the average level of ADMA was determined separately for each stage of DM type 2. In the patients with a mild form of DM type 2, the average level of ADMA was 0.43 ± 0.15 μmol/l; in patients with a moderate form of DM type, it was 2 – 1.27 ± 0.14 μmol/l, and those with a severe form of DM type 2 had a result of 1.97 ± 0.05 μmol/l (p < 0.05), as shown in Figure 3 and Table 2 .
The average level of troponin I on the first day of AMI in the patients of Group 1 was 4.89 ± 2.46 ng/ml, while for Group 2 it was 2.67 ± 2.06 ng/ml and for the reference group, 0.06 ± 0.04 ng/ml (р 1-2 ˂ 0.00001, р 1-3 ˂ 0.00001, p 2-3 < 0.00001), as shown in Table 3 .
The research undertaken determined the average level of troponin I for each stage of DM type 2 in the patients from Group 1. In the patients with a mild form of DM type 2, the average level of troponin I was 1.53 ± 1.03 ng/ml, while for those with a moderate form of DM type 2, it was 2.93 ± 1.91 ng/ml. The result for a severe form of DM type 2 was 7.04 ± 5.21 ng/ml (p < 0.005), as shown in Table 4 .
The direct marked correlation between ADMA and troponin I levels was revealed in the course of the correlation analysis (r = 0.687; p ˂ 0.05).
The correlation between ADMA and troponin I levels in the patients in Group 1 according to the stages of DM type 2 demonstrated the following results: between the indicators of patients with a mild form of DM type 2, there was found to be a direct marked correlation (r = 0.500; p > 0.05), between the indicators of patients with a moderate form of DM type 2 there was a direct strong correlation (r = 0.797; p ˂ 0.05), and between the indicators of patients with a severe DM type 2, there was a direct strong correlation (r = 0.757; p ˂ 0.05), as shown in Table 5 .
Discussion
In the course of this study, it was determined that the patients with AMI had an increased level of ADMA compared to individuals who were part of the control group. In patients with concomitant DM type 2, the level of ADMA was 2.57 times a higher than in the patients with isolated АМІ (p < 0.05). This indicates an even greater hyperactivity of the marker of endothelial dysfunction, ADMA, because it is this dysfunction that combines the pathogenesis of comorbid pathology. It should be noted that the level of ADMA is directly proportional to the stage of DM type 2.
The results of recent research associate ADMA with AMI prognosis. Researchers examined 66 patients with AMI, measuring their level of ADMA, symmetric dimethylarginine (SDMA), marker of myocardial damage (troponin T), and inflammation marker (C-reactive protein (CRP)) at the point of hospitalization (< 24 h) and on the third day of inpatient treatment. The results of the research demonstrated the following: the concentration of ADMA in the blood on the first day was positively correlated with registered daily sleep hours (r = 0.497; p ˂ 0.001) and the frequency of meals (r = 0.285; p < 0.05), while it was negatively correlated with the registered physical condition (r = -0.304; p = 0.013). Hypertension in the patient’s medical history indicated a higher concentration of ADMA on the first day of AMI in contrast to the patients without hypertension at 1.818 and 1.568, respectively (p < 0.05). The age of the patients who participated in this study was also positively correlated with SDMA on the first day of measurement (r = 0.320; p < 0.01). All concentrations of the biomarkers were reduced following repeated measurement on the third day of inpatient treatment (p < 0.001). A positive correlation was found between a normal body mass index (BMI) and both an absolute (r = 0.366; p < 0.01) and percentage (r = 0.262; p < 0.05) reduction in ADMA. Thus, modifiable factors (BMI, physical condition and sleep, and eating habits) affect the level of ADMA and SDMA within AMI patients. Other values of these factors can influence the prognosis of AMI by influencing the level of ADMA 42 , 43 , 44 .
When measuring the level of troponin I, in the examined persons it was found that in case of AMI, the level of this marker of myocardial damage was significantly higher than normal (up to 0.5 ng/ml) in contrast to the participants of the research who were in the reference group. The level of this indicator was directly proportional to the size of the necrosis. In the case where the patients had a carbohydrate disorder with insulin resistance and hyperglycemia in the form of DM type 2, the level of this indicator was almost two times higher than it was in patients with isolated AMI (p < 0.00001). When determining the level of the marker of myocardial necrosis (troponin I) in the patients in Group 1, it was found to be directly proportional to the stages of DM type 2.
Scientists examined 164 patients with decompensated chronic heart failure to assess the 30-day risk of mortality by determining the level of glucose, troponin, N-terminal pro-cerebral sodium naturetic peptide, creatinine clearance, and undertaking electrocardiogram analysis (ECG). The research found that the persons with a lethal outcome within 30 days had significantly elevated levels of N-terminal pro-cerebral sodium naturetic peptide, troponin, fasting glucose, creatinine clearance, and an abnormal ECG repolarization. That is, changes in the above parameters acted as the markers of a short-term risk of mortality among this group of patients 45 , 46 , 47 .
Mohebi R. et al . found there to be an association between the troponin I concentration and obstructive CHD. They examined 978 patients, and 607 patients (62%) from among that number had obstructive CHD. The highest concentration of troponin I was found in relation to CHD, chronic kidney disease, heart failure, high low-density lipoprotein, anemia, male gender, smoking, and advanced age. CHD in the patient’s medical history, being male, type 2 DM, hs-cTnI, anemia, advanced age, and high-density lipoprotein cholesterol were identified as the most influential factors for CHD. The gradient amplification model in this case had an area under the curve of 0.82, an accuracy level of 75%, sensitivity of 88%, specificity of 52%, positive predictive value of 76%, and negative predictive value of 72% as a predictor of CHD. The gradient amplification model in this study had an area under the curve of 0.82, accuracy of 75%, sensitivity of 88%, specificity of 52%, positive predictive value of 76%, and negative predictive value of 72% for predicting CHD. A 1 logarithmic unit increase in troponin I was significantly associated with an increased risk of AMI development (HR 1.34, 95% CI 1.22 to 1.47; p < 0.001), adverse cardiovascular events (HR 1.24, 95% CI 1.11 to 1.39; p < 0.001), as well as an increase in mortality from AMI and other unfavorable cardiovascular diseases (HR 1.29, 95% CI 1.20 to 1.40; p < 0.001). Researchers have shown that high concentrations of troponin I have been associated with CHD and a high risk of future cardiovascular events 48 , 49 , 50 .
Hjort M. et al. examined patients suffering from AMI with non-obstructive coronary arteries (MINOCA). This is a newly recognized condition for which the biomarkers and prognosis are less well studied than in АMI with obstructive coronary artery disease (MI-CAD). The research cohort consisted of 1,639 patients with MINOCA and 17,304 patients with MI-CAD. In the adjusted analyses, the troponin levels in MINOCA patients predicted all-cause mortality (HR 1.32, 95% CI 1.11 to 1.56), mortality due to cardiovascular events (HR 2.11, 95% CI 1.51 to 2.96), and serious cardiovascular events, also known as MACE (HR 1.44, 95% CI 1.20 to 1.72). A high level of troponin I also predicted re-hospitalization for cardiac failure (HR 1.51, 95% CI 1.51 to 2.96) but not for non-fatal AMI or stroke. The analysis showed that the troponin I level is the same prognostic marker for assessing the risk of mortality in patients with MINOCA compared to those with MI-CAD 51 .
During the correlation analysis, a direct marked correlation was revealed between the levels of ADMA and troponin I in general and a direct strong correlation between the above indicators in patients with moderate and severe forms of DM type 2. This indicates the relationship between the predictor dysfunction of the endothelium and the marker of myocardial damage.
Conclusions
Thus, asymmetric dimethylarginine acts as a marker of endothelial dysfunction. This has a high diagnostic value in the case of patients with acute myocardial infarction, especially when in combination with diabetes mellitus type 2. When the above diseases combined in patients, the level of asymmetric dimethylarginine was 2.57 times higher than in patients with resolved acute myocardial infarction (p < 0.05). This research has revealed the hyperactivity of the marker of myocardial damage, troponin I, in patients with acute myocardial infarction and diabetes mellitus type 2. In the combination the above conditions, the level of this indicator was almost twice as high as in the case of isolated myocardial infarction (p < 0.00001).
In the course of the correlation analysis, a direct marked correlation was found between the levels of asymmetric dimethylarginine and troponin I (p ˂ 0.05). When determining the above indicators in the patients of Group 1 as per the form of diabetes mellitus type 2, a direct proportional relationship was found between the studied parameters (in the case of the patients with a severe form of diabetes mellitus type 2, the levels of asymmetric dimethylarginine and troponin I were significantly higher than in the cases with mild and moderate forms of diabetes mellitus type 2 (p < 0.05)). Correlation analysis between the marker of endothelial dysfunction and the marker of myocardial damage in the patients of Group 1 as per the form of diabetes mellitus type 2 demonstrated a direct marked correlation in the case of a mild form of carbohydrate metabolism disorder and a direct strong correlation in the case of moderate and severe carbohydrate metabolism disorders.
Abbreviations
None.
Acknowledgments
None.
Author’s contributions
All authors equally contributed to this work. All authors read and approved the final manuscript.
Funding
None.
Availability of data and materials
Data and materials used and/or analyzed in the current study and available from the corresponding author upon reasonable request.
Ethics approval and consent to participate
The study was conducted in compliance with the basic bioethical provisions of the Council of Europe Convention on Human Rights and Biomedicine (March 4, 1997), the Helsinki Declaration of the World Medical Association on the ethical principles of scientific medical research involving humans (1964-2008), and the order of the Ministry of Health of Ukraine No./690 dated September 23, 2009.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
References
- Zhao D., Liu J., Wang M., Zhang X., Zhou M.. Epidemiology of cardiovascular disease in China: current features and implications. Nature Reviews. Cardiology. 2019;16(4):203-12. View Article PubMed Google Scholar
- Huang Z., Wu M., Zeng L., Wang D.. The Beneficial Role of Nrf2 in the Endothelial Dysfunction of Atherosclerosis. Cardiology Research and Practice. 2022;2022:4287711. View Article PubMed Google Scholar
- Fang E.F., Scheibye-Knudsen M., Jahn H.J., Li J., Ling L., Guo H.. A research agenda for aging in China in the 21st century. Ageing Research Reviews. 2015;24:197-205. View Article PubMed Google Scholar
- Roule V., Lemaitre A., Pommier W., Bignon M., Sabatier R., Blanchart K.. Safety and efficacy of very short dual antiplatelet therapy followed by P2Y12 inhibitor monotherapy in older patients undergoing percutaneous coronary intervention: meta-analysis of randomised controlled trials. Age and Ageing. 2021;50(4):1102-7. View Article PubMed Google Scholar
- Cui K., Yin D., Zhu C., Yuan S., Wu S., Feng L.. Optimal revascularization strategy for patients with ST-segment an elevation myocardial infarction and multivessel disease: a pairwise and network meta-analysis. Frontiers in Cardiovascular Medicine. 2022;8:695822. View Article PubMed Google Scholar
- Towashiraporn K., Krittayaphong R.. Current perspectives on antithrombotic therapy for the treatment of acute coronary syndrome. International Journal of General Medicine. 2022;15:2397-414. View Article PubMed Google Scholar
- Khalifa A.A., El Sokkary N.H., Elblehi S.S., Diab M.A., Ali M.A.. Potential cardioprotective effect of octreotide via NOXs mitigation, mitochondrial biogenesis and MAPK/Erk1/2/STAT3/NF-kβ pathway attenuation in isoproterenol-induced myocardial infarction in rats. European Journal of Pharmacology. 2022;925:174978. View Article PubMed Google Scholar
- Gerbaud E., Bouchard de La Poterie A., Baudinet T., Montaudon M., Beauvieux M.C., Lema\^\itre A.I.. Glycaemic Variability and Hyperglycaemia as Prognostic Markers of Major Cardiovascular Events in Diabetic Patients Hospitalised in Cardiology Intensive Care Unit for Acute Heart Failure. Journal of Clinical Medicine. 2022;11(6):1549. View Article PubMed Google Scholar
- Gerbaud E., Darier R., Montaudon M., Beauvieux M.C., Coffin-Boutreux C., Coste P.. Glycemic Variability Is a Powerful Independent Predictive Factor of Midterm Major Adverse Cardiac Events in Patients With Diabetes With Acute Coronary Syndrome. Diabetes Care. 2019;42(4):674-81. View Article PubMed Google Scholar
- Wang C., Kong Y., Ding Y., Sun J., Chen T.. Serum Calprotectin Levels and Outcome Following Percutaneous Coronary Intervention in Patients with Diabetes and Acute Coronary Syndrome. Medical Science Monitor. 2019;25:9517-23. View Article PubMed Google Scholar
- Winzap P., Davies A., Klingenberg R., Obeid S., Roffi M., Mach F.. Diabetes and baseline glucose are associated with inflammation, left ventricular function and short- and long-term outcome in acute coronary syndromes: role of the novel biomarker Cyr 61. Cardiovascular Diabetology. 2019;18(1):142. View Article PubMed Google Scholar
- Kap\lan C., Kalemba A., Krok M., Krzych \L.. Effect of Treatment and Nutrition on Glycemic Variability in Critically Ill Patients. International Journal of Environmental Research and Public Health. 2022;19(8):4717. View Article PubMed Google Scholar
- Park M.J., Choi K.M.. Association between Variability of Metabolic Risk Factors and Cardiometabolic Outcomes. Diabetes {&}amp; Metabolism Journal. 2022;46(1):49-62. View Article PubMed Google Scholar
- Yang Y., Hu Y.. Comment on Gerbaud et al. Glycemic Variability Is a Powerful Independent Predictive Factor of Midterm Major Adverse Cardiac Events in Patients With Diabetes With Acute Coronary Syndrome. Diabetes Care 2019;42:674-681. Diabetes Care. 2019;42(10):e168-9. View Article PubMed Google Scholar
- Huang G., Cheng Z., Hildebrand A., Wang C., Cimini M., Roy R.. Diabetes impairs cardioprotective function of endothelial progenitor cell-derived extracellular vesicles via H3K9Ac inhibition. Theranostics. 2022;12(9):4415-30. View Article PubMed Google Scholar
- Low Wang C.C., Hess C.N., Hiatt W.R., Goldfine A.B.. Clinical Update: Cardiovascular Disease in Diabetes Mellitus: Atherosclerotic Cardiovascular Disease and Heart Failure in Type 2 Diabetes Mellitus - Mechanisms, Management, and Clinical Considerations. Circulation. 2016;133(24):2459-502. View Article PubMed Google Scholar
- Badacz R., Przew\locki T., Pieni\każek P., Ros\lawiecka A., Kleczyński P., Legutko J.. MicroRNA-134-5p and the Extent of Arterial Occlusive Disease Are Associated with Risk of Future Adverse Cardiac and Cerebral Events in Diabetic Patients Undergoing Carotid Artery Stenting for Symptomatic Carotid Artery Disease. Molecules (Basel, Switzerland). 2022;27(8):2472. View Article PubMed Google Scholar
- Badacz R., Kab\lak-Ziembicka A., Ros\lawiecka A., Rzeźnik D., Baran J., Trystu\la M.. The Maintained Glycemic Target Goal and Renal Function Are Associated with Cardiovascular and Renal Outcomes in Diabetic Patients Following Stent-Supported Angioplasty for Renovascular Atherosclerotic Disease. Journal of Personalized Medicine. 2022;12(4):537. View Article PubMed Google Scholar
- Pantazi K., Karlafti E., Bekiaridou A., Didagelos M., Ziakas A., Didangelos T.. Insulin Receptors and Insulin Action in the Heart: The Effects of Left Ventricular Assist Devices. Biomolecules. 2022;12(4):578. View Article PubMed Google Scholar
- Bladowski M., Szahidewicz-Krupska E., Wiśniewski J., Fortuna P., Chojdak-\Lukasiewicz J., Budrewicz S.. Changes in the Plasma and Platelet Nitric Oxide Biotransformation Metabolites during Ischemic Stroke-A Dynamic Human LC/MS Metabolomic Study. Antioxidants. 2022;11(5):955. View Article PubMed Google Scholar
- Förstermann U., Xia N., Li H.. Roles of Vascular Oxidative Stress and Nitric Oxide in the Pathogenesis of Atherosclerosis. Circulation Research. 2017;120(4):713-35. View Article PubMed Google Scholar
- Wang Y., Hong F., Yang S.. Roles of Nitric Oxide in Brain Ischemia and Reperfusion. International Journal of Molecular Sciences. 2022;23(8):4243. View Article PubMed Google Scholar
- Cetin Z., Kosem A., Catak M., Can B., Baser O., Guler S.. The Relationship of Thyroid Functions with ADMA, IMA, and Metabolic Laboratory Parameters in Euthyroid Adults with and without Autoimmune Thyroiditis. Laboratory Medicine. 2022;53(3):290-5. View Article PubMed Google Scholar
- Lee F.Y., Luo C.W., Wallace C.G., Chen K.H., Sheu J.J., Yin T.C.. Direct implantations of erythropoietin and autologous EPCs in critical limb ischemia (CLI) area restored CLI area blood flow and rescued remote AMI-induced LV dysfunction. Biomedicine and Pharmacotherapy. 2019;118:109296. View Article PubMed Google Scholar
- Oikonomou E., Siasos G., Zaromitidou M., Hatzis G., Mourouzis K., Chrysohoou C.. Atorvastatin treatment improves endothelial function through endothelial progenitor cells mobilization in ischemic heart failure patients. Atherosclerosis. 2015;238(2):159-64. View Article PubMed Google Scholar
- Fang J., Guo Y., Tan S., Li Z., Xie H., Chen P.. Autologous Endothelial Progenitor Cells Transplantation for Acute Ischemic Stroke: A 4-Year Follow-Up Study. Stem Cells Translational Medicine. 2019;8(1):14-21. View Article PubMed Google Scholar
- Naseri M.H., Madani H., Ahmadi Tafti S.H., Moshkani Farahani M., Kazemi Saleh D., Hosseinnejad H.. COMPARE CPM-RMI Trial: Intramyocardial Transplantation of Autologous Bone Marrow-Derived CD133+ Cells and MNCs during CABG in Patients with Recent MI: A Phase II/III, Multicenter, Placebo-Controlled, Randomized, Double-Blind Clinical Trial. Cell Journal. 2018;20(2):267-77. View Article PubMed Google Scholar
- Ponikowska B., Iwanek G., Zdanowicz A., Urban S., Zymliński R., Ponikowski P.. Biomarkers of Myocardial Injury and Remodeling in Heart Failure. Journal of Personalized Medicine. 2022;12(5):799. View Article PubMed Google Scholar
- Mader M.M., Czorlich P.. The role of L-arginine metabolism in neurocritical care patients. Neural Regeneration Research. 2022;17(7):1446-53. View Article PubMed Google Scholar
- Mader M.M., Böger R., Appel D., Schwedhelm E., Haddad M., Mohme M.. Intrathecal and systemic alterations of L-arginine metabolism in patients after intracerebral hemorrhage. Journal of Cerebral Blood Flow and Metabolism. 2021;41(8):1964-77. View Article PubMed Google Scholar
- Qi H., Li Q., Jing J., Jing T., Liu C., Qiu L.. Construction of N-CDs and Calcein-Based Ratiometric Fluorescent Sensor for Rapid Detection of Arginine and Acetaminophen. Nanomaterials (Basel, Switzerland). 2022;12(6):976. View Article PubMed Google Scholar
- Akar E., Emon S.T., Uslu S., Orakdogen M., Somay H.. Effect of L-Arginine Therapy on Vasospasm: Experimental Study in Rats. World Neurosurgery. 2019;132:e443-6. View Article PubMed Google Scholar
- González-López M.A., Ocejo-Viñals J.G., López-Sundh A.E., Guiral S., Ruiz-Solana M., Mata C.. Biomarkers of endothelial dysfunction and atherosclerosis in hidradenitis suppurativa. The Journal of Dermatology. 2022;49(10):1052-6. View Article PubMed Google Scholar
- Bonnitcha P., Sullivan D., Fitzpatrick M., Ireland A., Nguyen V.L., Koay Y.C., Sullivan J. O.. Design and validation of an LC-MS/MS method for simultaneous quantification of asymmetric dimethylguanidino valeric acid, asymmetric dimethylarginine and symmetric dimethylarginine in human plasma. Pathology. 2022;S0031-3025(22):00121. View Article Google Scholar
- Rodionov R.N., Jarzebska N., Burdin D., Todorov V., Martens-Lobenhoffer J., Hofmann A.. Overexpression of alanine-glyoxylate aminotransferase 2 protects from asymmetric dimethylarginine-induced endothelial dysfunction and aortic remodeling. Scientific Reports. 2022;12(1):9381. View Article PubMed Google Scholar
- Schlesinger S., Sonntag S.R., Lieb W., Maas R.. Asymmetric and symmetric dimethylarginine as risk markers for total mortality and cardiovascular outcomes: A systematic review and meta-analysis of prospective studies. PLoS One. 2016;11(11):e0165811. View Article PubMed Google Scholar
- Surrer D.B., Fromm M.F., Maas R., König J.. L-Arginine and Cardioactive Arginine Derivatives as Substrates and Inhibitors of Human and Mouse NaCT/Nact. Metabolites. 2022;12(4):273. View Article PubMed Google Scholar
- Banjarnahor S., König J., Maas R.. Screening of commonly prescribed drugs for effects on the CAT1-mediated transport of L-arginine and arginine derivatives. Amino Acids. 2022;54(7):1101-8. View Article PubMed Google Scholar
- Huang X., Zhuang J., Yang Y., Jian J., Ai W., Liu C.. Diagnostic Value of Serum Chitinase-3-Like Protein 1 for Liver Fibrosis: A Meta-analysis. BioMed Research International. 2022;2022:3227957. View Article PubMed Google Scholar
- Porro B., Eligini S., Conte E., Cosentino N., Capra N., Cavalca V.. An Optimized MRM-Based Workflow of the l-Arginine/Nitric Oxide Pathway Metabolites Revealed Disease- and Sex-Related Differences in the Cardiovascular Field. International Journal of Molecular Sciences. 2022;23(3):1136. View Article PubMed Google Scholar
- Canty J.M.. Myocardial injury, troponin release, and cardiomyocyte death in brief ischemia, failure, and ventricular remodeling. American Journal of Physiology. Heart and Circulatory Physiology. 2022;323(1):1-15. View Article PubMed Google Scholar
- Chalioti V.M., Giannakoulis V.G., Papoutsi E., Megalou A., Kritikos K., Konstantopoulos P.. Dimethylarginines in acute myocardial infarction: association with lifestyle, sociodemographic, and somatometric factors. Journal of Family Medicine and Primary Care. 2020;9(12):6234-9. View Article PubMed Google Scholar
- Arlouskaya Y., Sawicka A., G\lowala M., Giebu\ltowicz J., Korytowska N., Ta\la\laj M.. Asymmetric Dimethylarginine (ADMA) and Symmetric Dimethylarginine (SDMA) Concentrations in Patients with Obesity and the Risk of Obstructive Sleep Apnea (OSA). Journal of Clinical Medicine. 2019;8(6):897. View Article PubMed Google Scholar
- Aydin S., Ugur K., Aydin S., Sahin İ., Yardim M.. Biomarkers in acute myocardial infarction: current perspectives. Vascular Health and Risk Management. 2019;15:1-10. View Article PubMed Google Scholar
- Piccirillo G., Moscucci F., Carnovale M., Corrao A., Diego I. Di, Lospinuso I.. Glucose dysregulation and repolarization variability markers are short-term mortality predictors in decompensated heart failure. Cardiovascular Endocrinology & Metabolism. 2022;11(3):e0264. View Article PubMed Google Scholar
- Cunha F.M., Cidade-Rodrigues C., Elias C., Oliveira D., Bettencourt P., Lourenço P.. Glucose variability predicts 6-month mortality in patients hospitalized with acute heart failure. Internal and Emergency Medicine. 2021;16(8):2121-8. View Article PubMed Google Scholar
- Gerbaud E., Bouchard de La Poterie A., Baudinet T., Montaudon M., Beauvieux M.C., Lema\^\itre A.I.. Glycaemic Variability and Hyperglycaemia as Prognostic Markers of Major Cardiovascular Events in Diabetic Patients Hospitalised in Cardiology Intensive Care Unit for Acute Heart Failure. Journal of Clinical Medicine. 2022;11(6):1549. View Article PubMed Google Scholar
- Mohebi R., Jackson L., McCarthy C.P., Murtagh G., Murphy S.P., Abboud A.. Relation of High-Sensitivity Cardiac Troponin I and Obstructive Coronary Artery Disease in Patients Without Acute Myocardial Infarction. The American Journal of Cardiology. 2022;173:16-24. View Article PubMed Google Scholar
- Walter J., du Fay de Lavallaz J., Koechlin L., Zimmermann T., Boeddinghaus J., Honegger U.. Using High-Sensitivity Cardiac Troponin for the Exclusion of Inducible Myocardial Ischemia in Symptomatic Patients: A Cohort Study. Annals of Internal Medicine. 2020;172(3):175-85. View Article PubMed Google Scholar
- Lima B.B., Hammadah M., Kim J.H., Uphoff I., Shah A., Levantsevych O.. Relation of High-sensitivity Cardiac Troponin I Elevation With Exercise to Major Adverse Cardiovascular Events in Patients With Coronary Artery Disease. The American Journal of Cardiology. 2020;136:1-8. View Article PubMed Google Scholar
- Hjort M., Lindahl B., Baron T., Jernberg T., Tornvall P., Eggers K.M.. Prognosis in relation to high-sensitivity cardiac troponin T levels in patients with myocardial infarction and non-obstructive coronary arteries. American Heart Journal. 2018;200:60-6. View Article PubMed Google Scholar