Open Access
Open Access Abstract
Background: Trace minerals are of vital importance in normal body functions. Dysregulation of these minerals may cause serious clinical complications. Hemodialysis patients are usually at risk of deficiency or excess of any of these minerals. This study aimed to evaluate the levels of several trace minerals and serum electrolytes in hemodialysis patients in Pakistan.
Methods: The serum of patients undergoing hemodialysis and controls was analyzed for serum electrolytes and trace element levels, and the data were subjected to statistical analysis.
Results: A statistically significant difference was determined in Na+ (p = 0.0123) and K+ (p = 0.0020). Our data showed no significant difference in Cl-, Ca++ and PO4+3 (p > 0.05). Moreover, the RFT of the control and cases showed a distinctive difference, with the highest variances in blood urea (p < 0.0001) and serum creatinine (p < 0.0001). However, the uric acid levels in the population yielded a significant difference (p < 0.0001).
Conclusion: The biomarkers under study show promising roles in the diagnosis and early prevention of hemodialysis and kidney failure. For more accurate results, a large-scale investigation is needed.
Introduction
Hemodialysis (HD) is an artificial cleaning of blood that utilizes osmosis and diffusion between blood and dialysate across a semipermeable membrane. The dialysate is usually prepared according to the regulated amounts of essential components, which include several nutrients and essential minerals, primarily sodium (Na + ), calcium (Ca ++ ), potassium (K + ) and carbonate and bicarbonate salts. HD patients are usually at risk of mineral deficiency due to dietary restrictions and removal of essential minerals from the blood, as there is no regulation in reabsorption of minerals.
Generally, HD is engaged in several kidney disorders, such as chronic kidney disease, diabetes mellitus, glomerulonephritis and renal failure, which lead to end-stage renal disease. Chronic kidney disease is related to urine abnormalities or damage to excretory renal function that causes loss of functional nephron 1 . Glomerulonephritis is actually an immune-mediated disorder that causes inflammation in the glomerulus and other parts of the kidney 2 . Glomerulonephritis causes end-stage renal failure. Acute and sustained inflammation damages glomeruli and causes kidney fibrosis 3 .
Depending upon the availability of resources, disease management, lifestyle, mental health and dietary factors, mortality rates vary between and within the regions. For instance, the mortality rates in Japan were 6.6%, 15.6% in Europe and 21% in the United States 4 . Additionally, the populations with complex comorbidities have higher rates of mortality. HD prevalence is also lower in rural India, where 60% of patients travel almost 25 km to reach the closest unit 5 , 6 .
Higher mortality rates in hemodialysis patients reflect lower quality of life, advanced age and associated comorbidities. This can be improved by engaging in physical activities and promoting psychosocial health, which ultimately can help in gaining muscle strength and delaying disease progression 7 , 8 .
Basic living functions require electrolytes such as Na + , Ca ++ and K + to maintain electrical neutrality in cells and generate and conduct action potentials in nerves and muscles. The deficiency of trace minerals leads to impairment of body functions, as zinc (Zn ++ ) works as a cofactor in more than 70 enzymatic pathways, such as angiotensin converting enzyme, carbonic anhydrase, alkaline phosphatase, copper-zinc superoxide dismutase, DNA and RNA polymerases and metallothionein 9 .
The aim of the present study was to evaluate the levels of several trace minerals and serum electrolytes in hemodialysis patients. This study also estimates the altered levels of these biomarkers (serum uric acid, S. creatinine, urea) in healthy and dialysis patients.
Methods
Subject Selection
The subjects included were all hemodialysis patients, irrespective of the disease stage or other parameters, from the nephrology ward of hospitals in different areas of Punjab from February to June 2022.
Blood Sampling
Probable sampling was performed by obtaining blood samples from 364 subjects. The blood was sent to a lab for testing of serum electrolytes and renal function tests. Different parameters in serum electrolytes test (SET) and renal function test (RFT) reports were compiled into a data sheet for further statistical analysis.
Selection of parameters
To acquire baseline data, medical records were checked. It includes serum electrolytes (sodium level, chloride level, potassium level) and RFT, which includes creatinine level, uric acid level, and urea level.
Statistical Analysis
A statistically significant difference was determined by T test by using GraphPad Prism for both groups.
Results
Male to Female Incidence
The whole cohort was divided into 2 groups, SET and RFT, with subgroups of patients and control subjects ( Table 1 ). There was a male to female ratio specified in the cohort, which indicates that the sampling was random.
Figure 1 . Comparison of serum electrolytes in HD patients and controls . ( a ) Cl - (p = 0.0123), ( b ) Na + (p = 0.0020), and (c) K + (p < 0.05) were higher in HD patients than in control groups.

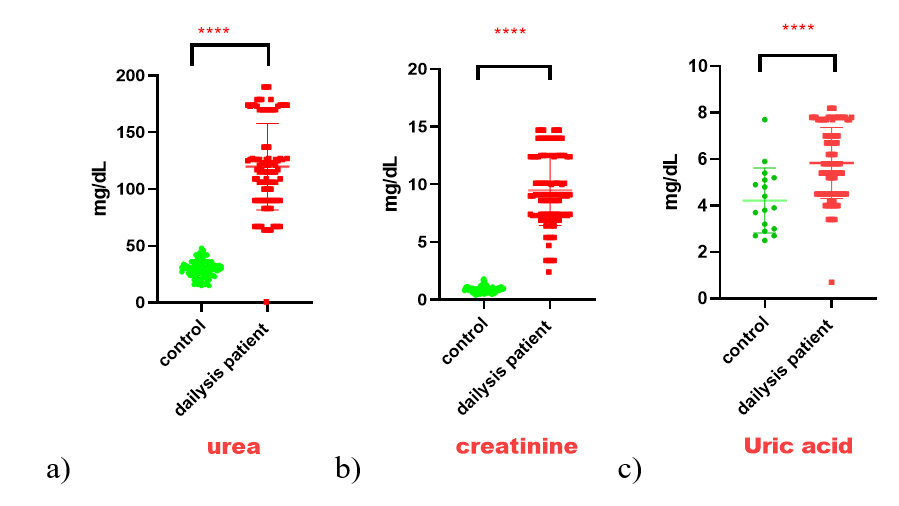
Figure 2 . Comparison of RFT reports between HD patients and controls . ( a ) Urea (p < 0.0001) and ( b ) creatinine (p < 0.0001) showed higher variance, whereas ( c ) uric acid (p < 0.0001) showed a significant difference between the groups.
Serum Electrolyses and Renal Function Parameters
A statistically significant difference was determined by t test on several trace minerals and serum electrolytes, including Na + (p = 0.0123), K + (p = 0.0020), Cl - , Ca ++ and PO 4 +3 (p < 0.05). This study shows deficient levels of various trace minerals and serum electrolytes in hemodialysis patients compared to healthy controls ( Figure 1 ). The RFT control and RFT patients showed a distinctive difference, with the highest variances in the blood urea (p < 0.0001) and serum creatinine (p < 0.0001) contents. However, the uric acid levels in the population yielded a significant difference (p < 0.0001) ( Figure 2 ).
SET and RFT Evaluation
Available information showed that blood creatinine, urea, and uric corrosive levels were higher, while Na + , K + , and Cl - levels were likewise higher but to a more modest extent in hemodialysis patients than in controls.
Discussion
The results show that serum sodium levels differ fundamentally. Lower blood salt levels are connected with specific hemodialysis patient attributes and an increased mortality risk. Further examination is important to decide if the lower casualty rate in dialyzed patients with serum sodium levels under 137 mEq/L contrasted with dialysate sodium solutions over 140 mEq/L is connected with intradialytic cardiovascular dependability 10 . In a consistent model, more prominent serum sodium levels were connected to diminished changed all-cause mortality (HR, 0.95 for each 1 mEq/L increase; 95% CI, 0.93-0.97). The solution for sodium dialysate was not connected with the serum sodium level. Patients with dialysate sodium remedies in excess of 140 mEq/L had a diminished mortality risk, as per mortality concentrates on that were restricted to the serum sodium tertile with the best mortality (serum sodium 137 mEq/L). In a nonstop model, higher serum sodium levels were connected to diminished changed all-cause mortality (HR, 0.95 for 1 mEq/L with dialysate sodium remedies > 140 mEq/L) 11 . The most common electrolyte issue is hyponatremia. At the point when the serum level of sodium is under 135 mmol/L, a condition is analyzed. The side effects of hyponatremia are neurological.
Our outcomes additionally show tremendous contrast in serum potassium. Heart arrhythmias are related to potassium issues. Low blood potassium levels, or hypokalemia, are portrayed by shortcomings, depletion, and jerking of the muscles. Arrhythmias might occur because of hyperkalemia, which occurs when blood potassium levels are over 5.5 mmol/L. Myoglobinuria, rhabdomyolysis, solid fits, and shortcomings are a portion of the side effects of hyperkalemia 12 . Both proximal and distal tubules (for the most part the proximal tubule) reabsorb most of the chloride that is separated by the glomerulus through dynamic and aloof vehicle. The deficiency of gastric bicarbonate could result in hyperchloremia. Hypochloremia can appear as regurgitating or gastrointestinal misfortunes or as a water maintenance condition such as congestive cardiovascular breakdown 13 . Heart arrhythmias are related to potassium issues. Arrhythmias might occur because of hyperkalemia, which occurs when blood potassium levels are over 5.5 mmol/L. Myoglobinuria, rhabdomyolysis, solid fits, and shortcomings are a portion of the side effects of hyperkalemia 12 .
Our outcomes likewise profoundly critical degree of serum creaitinine. Patients with CKD getting dialysis had serum creatinine levels up to 1.4 mg/dl more prominent than the typical reach. Prior to beginning hemodialysis, most patients have blood creatinine levels somewhere in the range of 7.6 and 12 mg/dl (57%) and 12 to 15 mg/dl (27%). Dialysis well affects serum creatinine levels, carrying them nearer to typical levels. Most patients (58%) had blood creatinine levels < 7 mg/dl following dialysis, as per the outcomes 14 . It is normally trusted that intense declines in renal capability/AKI are basically presumably causally associated with these results since larger expansions in serum creatinine ordinarily have a higher connection with these end focuses 15 .
Our outcomes additionally show massive contrast in serum chloride. It is just tracked down in the extracellular liquid compartment (ECF), which incorporates the interstitial liquid compartment and the blood/plasma (or serum) compartment. The primary anion associated with sodium in the ECF is chloride. The ordinary scope of serum chloride focuses is 96-106 mEq/L 13 . During the time of 1.7 long periods of middle development, expanded blood chloride was connected to a somewhat demolishing eGFR decline, free of other realized risk factors for CKD improvement. In demographically changed models, serum chloride was connected to an eGFR drop of over 30% however, the impacts were quieted and unimportant in totally amended models. Persistent models of serum chloride showed an association with eGFR drop for each 1 mEq/L ascent however, there was no conspicuous edge influence 16 .
Our results show tremendous contrast in serum urea and uric acid. Predialysis serum urea levels in CKD patients were extensively higher than the standard reach (20 – 40 mg/dl). Most of the patients (53%) had blood urea levels somewhere in the range of 200 and 300 mg/dl. After dialysis, serum urea levels altogether diminished; for most patients, they were between 1 – 100 mg/dl (26%) and 101 – 200 mg/dl (40%). The disposal of waste during dialysis is likewise affected by the planning of the methodology, patient mindfulness, and the dialyzer and diet decisions. It is often noticed that meat and salad greens might expand the weight of the kidneys and raise blood urea and creatinine levels 17 , 18 . In humans, including exogenous and endogenous purine metabolism, uric acid is the last oxidation product of purine catabolism 19 . One of the risk factors for renal disease, diabetes, and hypertension is hyperuricemia 20 . In addition, obesityand chronic heart failure can raise the risk of death from all causes when uric acid levels are high 21 . Uric acid is eliminated in the urine in two-thirds of cases 22 . Individuals with CKD usually have elevated uric acid levels due to reduced renal function. According to meta-analyses of CKD patients, higher SUA levels are substantially connected to an increased risk of cardiovascular death, revealing a U-shaped association between SUA and all-cause mortality 23 . The current primary results are limited to a smaller cohort size and simple criteria of inclusion. A more accurate approach can be adapted to produce more accurate results for the validation of these biomarkers in hemodialysis.
Conclusions
The parameters included in this study are promising markers to diagnose and possibly better understand renal functions. Both blood urea and serum creatinine levels display the most contrasting outcomes, thus signifying their roles.
Abbreviations
BUN : Blood urea nitrogen, CKD : chronic kidney disease, CVD : Cardiovascular disease, CVH : continuous venous hemofiltration, ECF : Extracellular fluid, ESRD : End-stage renal disease, GFR : Glomerular filtration rate, HD : Hemodialysis, RFT : renal function test, SET : Serum electrolyte Test, SUA : Serum uric acid
Acknowledgments
The authors are thankful to the Vice Chancellors of University of Narowal, Narowal, Pakistan, University of Okara, Punjab, Pakistan, and University of the Punjab, Lahore, Pakistan for providing the platform for the accomplishment of this study.
Author’s contributions
Khawar M B proposed the idea and supervised the work. Riasat M, Habiba U, and Afzal A wrote the manuscript and validated the first draft. Shahzaman S, Hamid S E and Aman S analyzed the data and interpreted the results. Abbasi M H, Sheikh N and Shah S S edited and revised the final manuscript. Idnan M, Tahir A, Butt A J and Tanveer S revised and approved the final manuscript. All authors read and approved the final manuscript.
Funding
None.
Availability of data and materials
Data are available on request.
Ethics approval and consent to participate
This study was conducted in accordance with the amended Declaration of Helsinki. The institutional review board approved the study, and all participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
References
- Romagnani P., Remuzzi G., Glassock R., Levin A., Jager K.J., Tonelli M.. Chronic kidney disease. Nature Reviews. Disease Primers. 2017;3(1):17088. View Article PubMed Google Scholar
- Chadban S.J., Atkins R.C.. Glomerulonephritis. Lancet. 2005;365(9473):1797-806. View Article PubMed Google Scholar
- Toda N., Mukoyama M., Yanagita M., Yokoi H.. CTGF in kidney fibrosis and glomerulonephritis. Inflammation and Regeneration. 2018;38(1):14. View Article PubMed Google Scholar
- Goodkin D.A., Bragg-Gresham J.L., Koenig K.G., Wolfe R.A., Akiba T., Andreucci V.E.. Association of comorbid conditions and mortality in hemodialysis patients in Europe, Japan, and the United States: the Dialysis Outcomes and Practice Patterns Study (DOPPS). Journal of the American Society of Nephrology. 2003;14(12):3270-7. View Article PubMed Google Scholar
- Hossain S., Sadik Batcha M.. Scientometric analysis of research productivity from Indian dialysis over the last twenty years in Web of Science. COLLNET Journal of Scientometrics and Information Management.. 2021;15(2):323-39. View Article Google Scholar
- Hazra A., Mandal S., Chakraborty J.. Tropical Journal of Pathology and Microbiology. Tropical Journal of Pathology and Microbiology.. 2021;7(1):18. Google Scholar
- Athienites N.V., Miskulin D.C., Fernandez G., Bunnapradist S., Simon G., Landa M.. Comorbidity assessment in hemodialysis and peritoneal dialysis using the index of coexistent disease. Seminars in Dialysis. 2000;13(5):320-6. View Article PubMed Google Scholar
- Wu Y.H., Hsu Y.J., Tzeng W.C.. Physical Activity and Health-Related Quality of Life of Patients on Hemodialysis with Comorbidities: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022;19(2):811. View Article PubMed Google Scholar
- Rucker D., Thadhani R., Tonelli M.. Trace element status in hemodialysis patients. Wiley Online Library; 2010.
- Hecking M., Karaboyas A., Saran R., Sen A., Hörl W.H., Pisoni R.L.. Predialysis serum sodium level, dialysate sodium, and mortality in maintenance hemodialysis patients: the Dialysis Outcomes and Practice Patterns Study (DOPPS). American Journal of Kidney Diseases. 2012;59(2):238-48. View Article PubMed Google Scholar
- Li H., Wang Y., Xu Y., Wu K., Lu X., Qiu Y.. Association between serum chloride levels with mortality in incident peritoneal dialysis patients. Nutrition, Metabolism, and Cardiovascular Diseases. 2022;32(3):624-31. View Article PubMed Google Scholar
- Viera A.J., Wouk N.. Potassium Disorders: hypokalemia and Hyperkalemia. American Family Physician. 2015;92(6):487-95. PubMed Google Scholar
- Morrison G.. Serum Chloride. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. Boston: Butterworths. . 1990;:. Google Scholar
- Lascano M.E., Poggio E.D.. Kidney function assessment by creatinine-based estimation equations. Current Clinical Medicine: Elsevier; 2010. p. 814-7. e1. . 2010;:. View Article Google Scholar
- Wald R., Quinn R.R., Luo J., Li P., Scales D.C., Mamdani M.M., University of Toronto Acute Kidney Injury Research Group Chronic dialysis and death among survivors of acute kidney injury requiring dialysis. Journal of the American Medical Association. 2009;302(11):1179-85. View Article PubMed Google Scholar
- Grodin J.L., Simon J., Hachamovitch R., Wu Y., Jackson G., Halkar M.. Prognostic role of serum chloride levels in acute decompensated heart failure. Journal of the American College of Cardiology. 2015;66(6):659-66. View Article PubMed Google Scholar
- Kaysen G.A., Greene T., Larive B., Mehta R.L., Lindsay R.M., Depner T.A., Trial Group FHN. The effect of frequent hemodialysis on nutrition and body composition: frequent Hemodialysis Network Trial. Kidney International. 2012;82(1):90-9. View Article PubMed Google Scholar
- Yazar H., Balci M., Basarali K.M., Gocmen A.Y., Buyukbas S.. The effects of dialysers on some blood biochemical parameters in hemodialysis patients. African Journal of Pharmacy and Pharmacology. 2011;5(22):2513-6. Google Scholar
- Tedeschi A., Agostoni P., Pezzuto B., Corra' U., Scrutinio D., La Gioia R.. Role of comorbidities in heart failure prognosis Part 2: chronic kidney disease, elevated serum uric acid. European Journal of Preventive Cardiology. 2020;27(2{_}suppl):35-45. View Article PubMed Google Scholar
- Johnson R.J., Bakris G.L., Borghi C., Chonchol M.B., Feldman D., Lanaspa M.A.. Hyperuricemia, acute and chronic kidney disease, hypertension, and cardiovascular disease: report of a scientific workshop organized by the National Kidney Foundation. American Journal of Kidney Diseases. 2018;71(6):851-65. View Article PubMed Google Scholar
- Stubnova V., Os I., H∅ieggen A., Solbu M.D., Grundtvig M., Westheim A.S.. Gender differences in association between uric acid and all-cause mortality in patients with chronic heart failure. BMC Cardiovascular Disorders. 2019;19(1):4. View Article PubMed Google Scholar
- Jalal D.I., Chonchol M., Chen W., Targher G.. Uric acid as a target of therapy in CKD. American Journal of Kidney Diseases. 2013;61(1):134-46. View Article PubMed Google Scholar
- Zhang J., Lu X., Li H., Wang S.. Serum uric acid and mortality in patients with chronic kidney disease: a systematic review and meta-analysis. Blood Purification. 2021;50(6):758-66. View Article PubMed Google Scholar